Considerations on the listening test
Considerations on the listening test — Antwerp 1973 / Amiens 1974
Fundamental document by Dr A. A. Tomatis, a printing of forty-eight pages published by the Société d’Audio-Psycho-Phonologie (4 rue Cozette, 80000 Amiens) in June 1974. This volume gathers the remarks made by Tomatis at the 3rd International Congress of Audio-Psycho-Phonology (Antwerp 1973), following a long question-and-answer exchange with his pupils. The work first presents the administration of the listening test (search for thresholds in air and bone conduction, study of spatialisation, study of selectivity, search for the dominant ear by audio-laterometer), then sets out — in twenty-two questions — the clinical and symbolic interpretation of the test: ideal physiological curve, tripartition viscerality / language / spirituality, maternal reading (left ear) and paternal reading (right ear), somatic correspondences (125 Hz = sexuality, 250 Hz = colon, 500 Hz = small intestine, 1,000 Hz = stomach …), differential diagnosis of conduction, perception and mixed deafnesses, reading of the depressive’s curves, and high-frequency listening postures. A permanent reference work of the practitioner for fifty years.
*CONSIDERATIONS ON THE LISTENING TEST
by
A. A. TOMATIS
SOCIÉTÉ D’AUDIO-PSYCHO-PHONOLOGIE
4, rue Cozette — 80000 Amiens
June 1974*
Remarks gathered in the course of the 3rd International Congress of Audio-Psycho-Phonology (Antwerp 1973) following an interview with Professor Tomatis.
In his work “Éducation et Dyslexie”, Professor Tomatis presented the listening test as the most important test of the audio-psycho-phonological assessment and as the one that must determine the listening possibilities of the subject: self-listening and listening to the other. In the pages he devoted to it in the chapter titled “Audio-Psycho-Phonological Assessment”, he defined the various tests composing this examination. We shall therefore only briefly recall what they consist in and how they are carried out.
For fuller details, we refer the reader to Professor Tomatis’s work “Éducation et Dyslexie”, Éditions ESF, “Sciences de l’Éducation” collection.
I. — Administration of the listening test
a) Search for thresholds
To carry out this test, we use a device containing a frequency generator called the “Hearing Test”, emitting pure tones from 125 to 8,000 hertz, from octave to octave, passing through the values 1,500, 3,000 and 6,000 hertz, the intensity of which may vary by 5 dB steps, from –10 to +100 dB.
This test aims to determine 4 parameters:
It is a matter of seeking on the one hand the minimum thresholds of audibility in air conduction, the sound entering the external canal of the ear via headphones; and on the other the thresholds obtained by bone conduction with the help of a vibrator that excites the mastoid. The results are recorded on two grids corresponding to the curve of the right ear and that of the left ear. It should be noted that the place of these two diagrams is inverted, the right curve being on the left and the left curve on the right, following an observation process usually applied in physiology.
On the abscissae are the frequencies from 125 to 8,000 hertz, and on the ordinates the intensities in decibels read from top to bottom. One thus obtains two air curves, that of the right ear and that of the left ear, generally represented in blue, and two bone curves traced generally in red pencil. When no colours are used, the air curve (CA) is indicated in solid line and the bone curve (CO) in dotted line.
b) Study of spatialisation
In the search for thresholds, one notes at the same time the ear’s power to locate sounds in space. Inversions or confusions of sounds are noted at the level of each frequency by a small line placed at the bottom of each of the grids. To collect these confusions or inversions of sounds, the subject is asked, during the search for thresholds, to raise the hand on the side where he hears the sound, and to raise both hands when he hears the sound on both sides or when he cannot determine the direction.
c) Study of selectivity
This investigation aims to detect the opening or closing of auditory selectivity. This selectivity has been defined by Professor Tomatis as the faculty an ear possesses of perceiving a variation of frequencies within a sound spectrum, and of locating the direction of this variation.
To carry out this test, one performs for each ear, in air conduction, and at a level of about 40-60 decibels, a sweep of frequencies, starting generally from the highs, and the subject is asked to indicate whether the sound perceived is higher, lower or of the same pitch as the preceding one.
The errors are indicated at the top of the grid, at the level of the poorly analysed frequencies, and the blockage of selectivity is indicated by hatched lines from the lowest frequency that has been marked with a line.
d) Search for the dominant ear
The last test of the listening test is carried out with the help of the audio-laterometer. This study makes it possible to measure, to quantify the degree of lateralisation of the subject. It is in his work “Éducation et Dyslexie” that Professor Tomatis describes the audio-laterometer and its use (page 129). We shall not return to it here, contenting ourselves with pointing out that two figures are indicated on the diagram, that of the left ear (that is to say the one on the right) varying according to auditory lateralisation. If this is in favour of the left ear, we shall have on the diagram corresponding to this ear (that is, the diagram on the right) a figure going from 10 to 40. When this figure is at 50, there is no auditory dominance. When it is greater than 50, it is the right ear that dominates.
Thus, after the administration of the listening test, we find ourselves in the presence of two grids each containing two curves, one blue and one red (or one solid-line curve and one dotted-line curve), completed by the indication of inversions or confusions of sounds, by data on selectivity, and at the same time by two figures corresponding to the audio-laterometer test.
Recording this test correctly is not sufficient. It must then be interpreted properly, which requires long practice.
II. — Interpretation of the listening test
This approach is difficult to carry out. It is one of the parts of Professor Tomatis’s theories and research at once the most complex and yet wholly primordial for the proper application of the techniques used in the domain of Audio-Psycho-Phonology.
We shall, by alternating questions and answers, nevertheless try to clarify and circumscribe the problem.
First question
Could you define exactly what you mean by a listening test and indicate to us what fundamental differences there may be between a listening test and an audiogram?
Professor Tomatis: I think indeed that there exists an important difference between an audiogram and a listening test. The material the latter brings on various planes makes it possible to group together a considerable quantity of elements that give the informed clinician a precious substance for establishing the diagnosis.
This test differs from the simple audiogram, which somehow measures the subject’s audition. This last result interests us, to be sure, but it is not the essential element sought. Indeed, I repeat once more that one must clearly distinguish listening from audition. To hear does not imply for all that the presence of a conscious field. To hear is somehow to undergo a sound or a message addressed to us. To listen is to wish to apprehend this sound or this message. They are two different postures.
Audiometry is certainly not to be neglected, but the spirit in which it is carried out can make the interpretations vary according to the clinical or psychological contribution it is capable of putting at our disposal. This test remains essential in the matter of investigations bearing on audition. It is for the otologist a fundamental examination from which the aetiological data of an auditory disorder take shape. On it depends, moreover, the prognosis that will orient the mode of medical or surgical therapy, or even prosthetic, even re-educational. One may therefore, from these data, apply the rules of care intended to re-establish a damaged function.
The listening test knows how to integrate this information within the framework of a psychological process that will make it possible to detect whether the subject wishes or does not wish to use the materials at his disposal on the perceptive plane. Everyone knows these so often reiterated leitmotifs: “they have ears and do not hear; they hear but they do not know how to listen”. There is a gradation that institutes itself between hearing and listening; and the listening test makes it possible precisely to know the use a subject is able to make of his audition. The audiogram gives a determined curve but does not indicate whether the individual examined really knows how to use this curve to communicate with others through his self-control. In matters of vision, you have the same gradations. You may find yourself before a perfect eye, before the best retina in the world; that will not however allow you to detect whether the subject knows how to aim well with a rifle or whether he knows how to paint. There exists therefore a dimension of gnosis that brings a complementary datum. Thus, in Audio-Psycho-Phonology, one observes that a poor curve can be very well used and bring the subject listening possibilities of which many well-hearing people are deprived. I have seen people who, on the basis of their audiogram, are considered deaf and who nevertheless manage to listen by fixing their attention. There is therefore a dimension of attention, of adhesion, that institutes itself in listening, a coming-to-consciousness that interlocks with audition itself. The listening test therefore is situated at a higher level than that of the audiogram itself. It is above all a psychological test, while the audiogram remains a test of a physiological — indeed anatomical — order.
Second question
You therefore consider that there is an essential difference between hearing and listening?
Professor Tomatis: Yes, I think it is necessary to know how to discern these two essentially distinct functions, although evolving apparently on identical terrains. While it is true that both these faculties cover the same territory, it is no less true that they diverge in their mode of action, according to the underlying motivations. To hear is the result of a perception responding to a stimulation coming from outside. To listen is based, to be sure, on a stimulation taking its source on the outside, but having to be inwardly, intentionally sought. The notions of sensor, of choice, of filter, then appear. The conscious element thus becomes the essential factor on which rests the whole difference between these two activities that evolve in parallel and of which one, listening, is situated on a higher plane, since it calls upon a specific characteristic of man in his human course.
To see and to wish to see are two wholly different mechanisms, the second using the first. To wish to see is to aim. It is the same for hearing and listening. Listening results from the wish to hear and is the equivalent of aiming. Listening is to the ear what aiming is to the eye. This distinction must be constantly present in the mind of the audio-psycho-phonologist. It is for him to know, through the results that pure audiology offers him, how to safeguard the psychological data that will allow him to establish his diagnosis and to orient his mode of action.
Third question
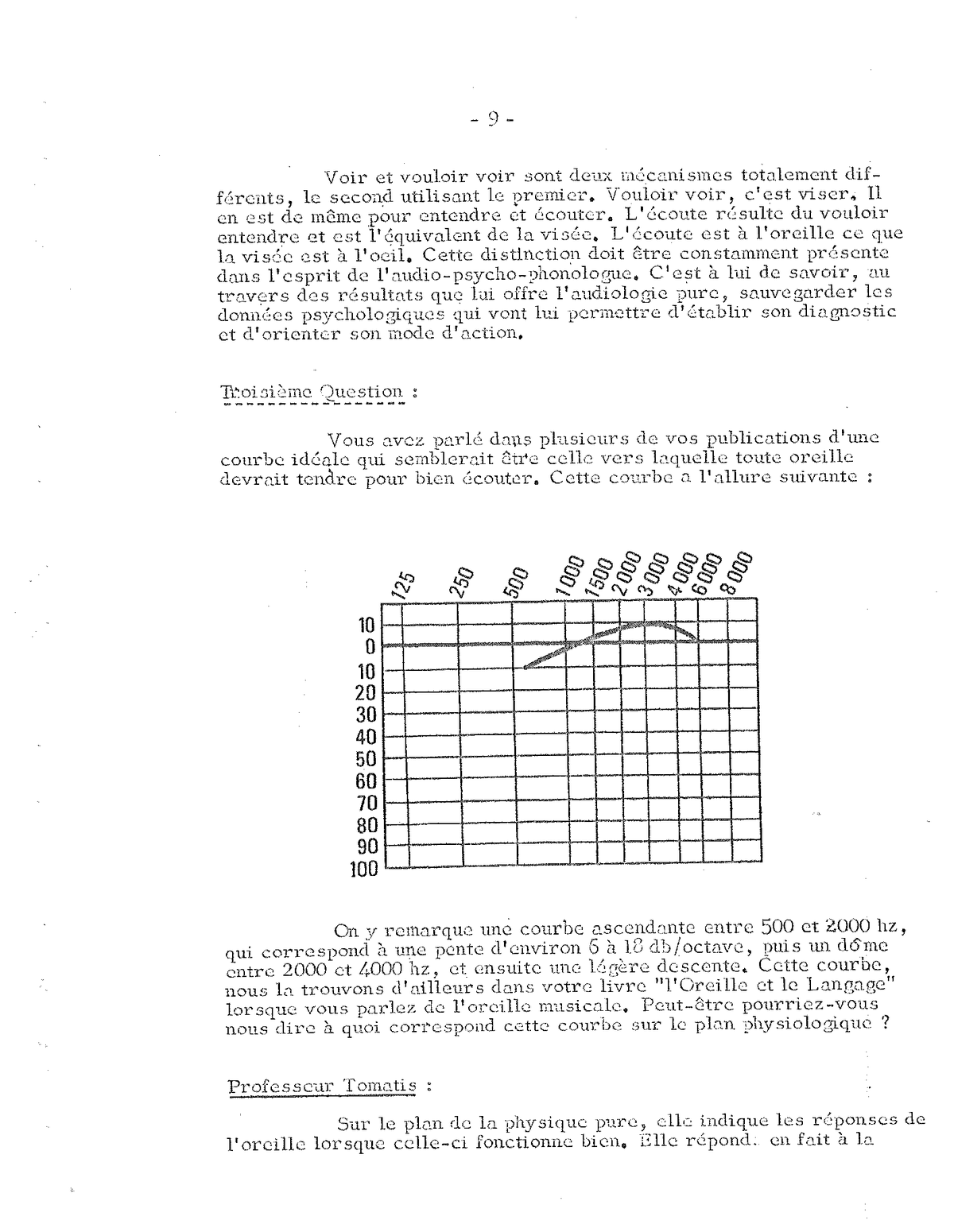
You have spoken in several of your publications of an ideal curve that would seem to be the one towards which any ear should tend in order to listen well. This curve has an ascending shape between 500 and 2,000 Hz, corresponding to a slope of about 6 to 18 dB/octave, then a dome between 2,000 and 4,000 Hz, and then a slight descent. This curve we find moreover in your book “L’Oreille et le Langage” when you speak of the musical ear. Perhaps you could tell us what this curve corresponds to on the physiological plane?
Ideal physiological curve: regular ascent between 500 and 2,000 Hz (slope of about 6 to 18 dB/octave), dome between 2,000 and 4,000 Hz, slight descent thereafter.
Professor Tomatis: On the plane of pure physics, it indicates the ear’s responses when the latter is functioning well. It corresponds, in fact, to the Wegel curve, called the “lemon-shaped curve”, inverted. Indeed, the Wegel curve is the response curve obtained when frequencies are placed on the abscissa and ascending intensities on the ordinate. A first threshold is obtained, in the lower part, following a minimum that begins in the low frequencies at about 40-50 dB, then approaches the curve of the abscissa between 2,000 and 3,000 Hz and becomes ascending again at 40-50 dB in the highs between 8 and 10,000 Hz. This curve is completed and takes the shape of a lemon — according to the figurative expression conferred on it when one sends sounds of increasing intensity and one then obtains a curve of maximum thresholds, determined where the ear begins to suffer, whence the name “thresholds of pain”.
Wegel curve, the so-called “lemon curve”: field of audibility bounded below by the threshold of audibility and above by the threshold of pain.
These thresholds begin in the lows also at 50-60 dB, rejoining the first curve, then they reach 120 to 130 dB between 2,000 and 3,000 Hz to then fall in the highs, also rejoining the first curve.
The median line, which lies at about 50-60 dB, which is linear, represents a zone called the “Munsen zone”. It answers to the dynamic of the ear, that is to say to its optimum zone of functioning without distortions. In all other zones, as one can see, the ear acts as a filter whose slopes are variable according to intensity, with a rotation point situated between 1,000 and 2,000 Hz. To make up for these distortions, always difficult to integrate in the reading of the diagrams, the Americans have standardised the audiograms of the type we all use, by inverting Wegel’s image and by straightening the minima to obtain a straight line. These standards nevertheless keep a preferential zone between 1,000 and 2,000 Hz (the bump we know well) despite the compensations of 30 to 40 dB granted on the curve, in the lows and highs.
There exists therefore a kind of ideal physiological curve that should be sought. But do not believe that, when you have acquired it, it will be given to you to reach the conscious field. However, it is sure that if you do not have this exceptional ear, you risk not being a musician, not being able to reproduce sounds of quality. If a violinist does not have this ear, he will not be able to play. In other words, it is indispensable for one who must reach a certain plane, but it is not sufficient.
I therefore think it is a physico-acoustic response curve whose presence is necessary for the elaboration of the listening processes. Why does it not exist in all individuals? In fact, children come into the world with it as potentiality. But the dramas of life, the affective flicks, parental and social interdicts, and sometimes physiological miseries cause the child to close himself off from the world of listening, from the universe of communication. In his desire to listen no more, he introduces distortions, fadings; he lengthens the response circuits to be able to distance himself from those who make him suffer, from those he does not wish to encounter. But he remains prisoner of his “tricks”, of his stratagems that allowed him, at a given moment, to defend himself against the aggressions of the outside world. He will thus find himself shut in a closed space from which he can no longer come out. On the plane of the listening test, one then observes distortions, lacks compared to the ideal curve subjacent in every individual. It is therefore a question of straightening these distortions, of suppressing these lacks, by appropriate techniques intended to free the being imprisoned in his chains of non-listening.
The acquisition of this ideal curve corresponds to the harmonisation of the play of two muscles of the middle ear, allowing the permanent regulation of the internal pressure of the labyrinthine vesicle by bringing into play the phenomena of least impedance. In electro-acoustics or in mechanics, “impedance” is the process of minimum resistance. There is therefore reason to find, all along the course of sound through the ear, places of minimum impedance allowing the obtaining of an ideal response. Now, it happens that the whole auditory apparatus, from the external canal to the inner vesicle, responds to this ideal curve. It is one of the marvels of nature, one more! The human ear is therefore made, adapted, modelled to hear and to listen. The distortions that install themselves, the blockages that institute themselves, the deficiencies that appear are only there to slow motivation, to prevent exchange, to perturb dialogue, to trouble communication.
Fourth question
If one listens in this ideal way, which corresponds to a certain tension of the muscles of the hammer and the stirrup, one obtains, according to your writings, a damping of the lows and a fine perception of the highs. What therefore is the role of the eardrum in these listening processes?
Professor Tomatis: The eardrum sets itself in a certain state of tension to play the role of a tuning fork that makes the whole cranial box vibrate through the sulcus tympani. It is the whole cranial box that vibrates and transmits the sound to the labyrinthine vesicle, and not the ossicular chain that one is accustomed to consider as the vehicle of sound. The ossicular chain is a set that plays the role of adaptor, of regulator, and not of transmitter.
The conduction of sound by air and then by bone must therefore be studied in a complementary way so that one may subsequently determine the subject’s listening posture.
Fifth question
What difference is there therefore between the air curve and the bone curve?
Professor Tomatis: You do well to ask me this question, which is very important. I shall answer you at once that the air curve makes it possible to specify the way in which the subject listens to the outside world and in particular to the other, his interlocutor, the one speaking to him. The bone curve gives information on the way in which the subject listens to his inner life, his vegetative universe, his consciousness. It is the curve of self-listening, of self-control, of inner listening.
In fact, there should be only one curve corresponding to the junction of the two listenings: outer listening and inner listening. There is in reality only one true ideal curve. The calibrations of the two curves (air and bone) have been voluntarily shifted to be able to distinguish the different responses and interpret the distortions. When listening is perfect, the air and bone curves merge, but to facilitate the analysis of the results, parallel curves have been determined, the air curve having to be above the bone curve.
Listening ideal: the air curve (CA) should lie above the bone curve (CO), parallel to one another. Any air-bone gap reveals a dilemma between outer listening and self-listening.
It is plain that this result is rarely acquired. One most often observes distortions between the two curves, and these gaps are very interesting to observe. I really regret that, among the audition specialists, many do not pay attention to these differences, which nevertheless bring very precious elements for the establishment of the diagnosis. When there is distortion between the two listenings, when there is therefore a problem inside the being himself, one observes irregular gaps between air and bone conduction, indicating that the subject hears from the outside differently than for his inner life. There is a shift; there is a dilemma. One may find oneself before a very good outer-listening curve (air conduction) and have in self-listening (bone conduction) important distortions; vice versa, perturbations may be drawn at the level of air conduction while bone conduction indicates an inner listening of great quality. It is therefore important to study the relative position of one curve compared to the other, the air-bone gaps (CA/CO) translating in this case compensations.
Sixth question
What therefore is the attitude to take before a listening test on the plane of interpretation? What information can the air curve and the bone curve bring us, and what considerations can be retained from the study of the diagram of the right ear and that of the left ear?
Professor Tomatis: It is plain that this analysis can only be done globally, almost instantaneously, following great practice. It is with the listening test as with all other tests. Its interpretation requires a long, patient, meticulous apprenticeship for the global vision of what this test is able to bring to be outlined beyond the accumulation of information collected. In fact, with time, the experienced tester must be able at a single glance to grasp the totality of the successive planes outlined under the schema of the curves obtained, so that a synthesis may permit the necessary conclusions to be established. But is this not characteristic of all tests used in psychology?
Before a listening test, several parameters must therefore be considered and their relations among themselves studied. We shall begin by taking a few, the analysis of which we shall deepen by precise examples. We are thus in the presence of various data which I take the liberty of recalling to you:
-
air curve (CA)
-
bone curve (CO)
-
relation between CA and CO for each ear
-
relation between CA and CO from one ear to the other.
To go further into this interpretation work, we shall broach new elements of analysis bearing on the one hand on the signification of the left-ear diagram (the one on the right on our schemas) and of the right-ear diagram (on the left on the schemas), and on the other on the tripartition of each of the diagrams according to frequencies.
1°) Signification of the right and left diagrams
-
Everything relating to the left ear corresponds to affectivity, attachment to the past, the mother. The left is the mother, you have known that for a long time.
-
Everything relating to the right ear corresponds to dynamism, becoming, the father. The right is the father; here too I am telling you nothing new.
2°) Bringing to light different zones within each diagram
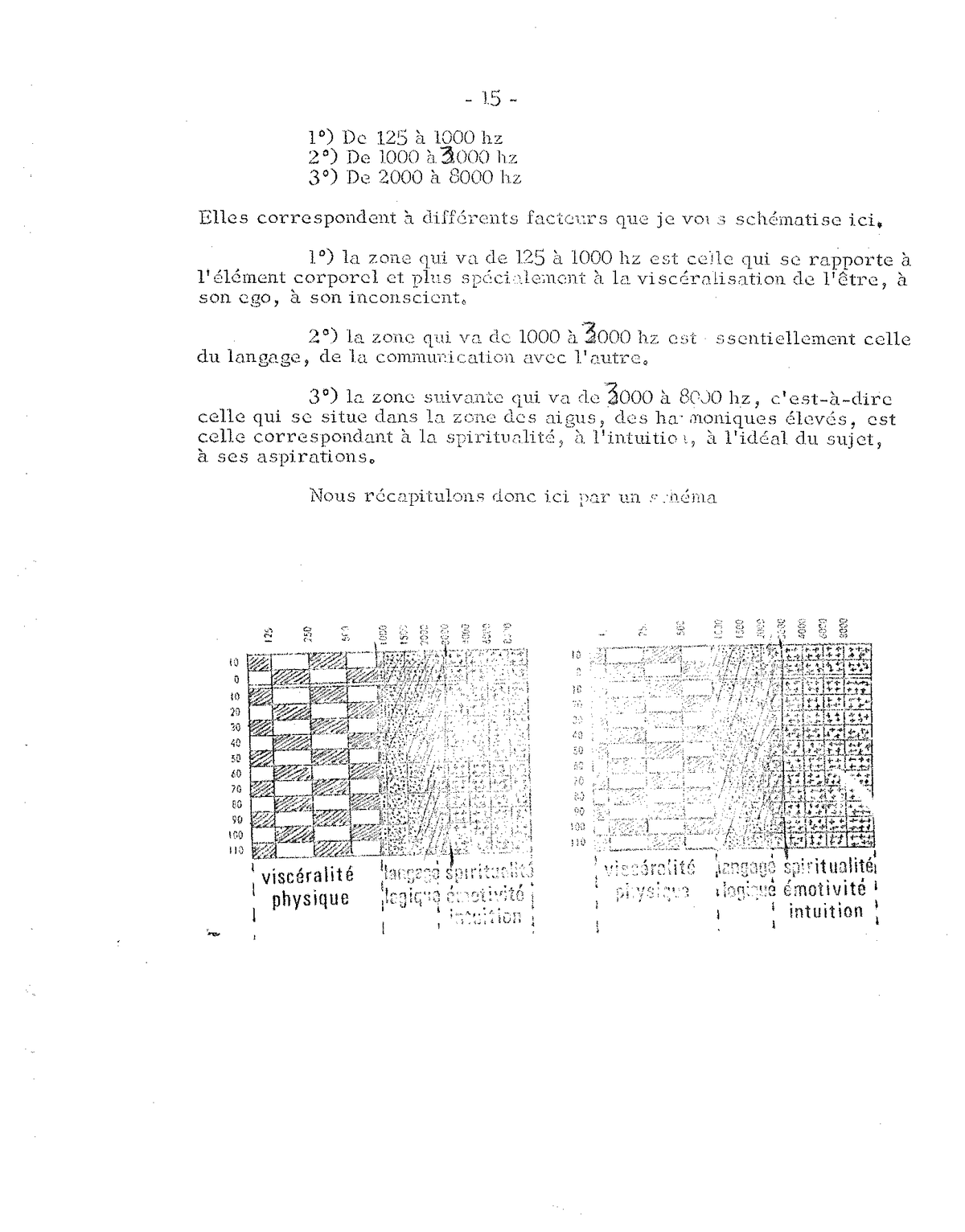
There is reason to divide each diagram into three zones we shall study successively from 125 to 8,000 Hz. These sound bands are distributed as follows:
-
From 125 to 1,000 Hz
-
From 1,000 to 3,000 Hz
-
From 2,000 to 8,000 Hz
They correspond to different factors that I schematise for you here.
-
the zone from 125 to 1,000 Hz is the one relating to the corporeal element and more especially to the visceralisation of the being, to his ego, to his unconscious.
-
the zone from 1,000 to 3,000 Hz is essentially that of language, of communication with the other.
-
the following zone, from 3,000 to 8,000 Hz — that is, the one in the zone of the highs, of the high harmonics — corresponds to spirituality, to intuition, to the subject’s ideal, to his aspirations.
Frequential tripartition of the two diagrams: physical viscerality (125-1000 Hz), language / logic / emotivity (1000-3000 Hz), spirituality / intuition (3000-8000 Hz).
3°) Clarifications on the zone of viscerality
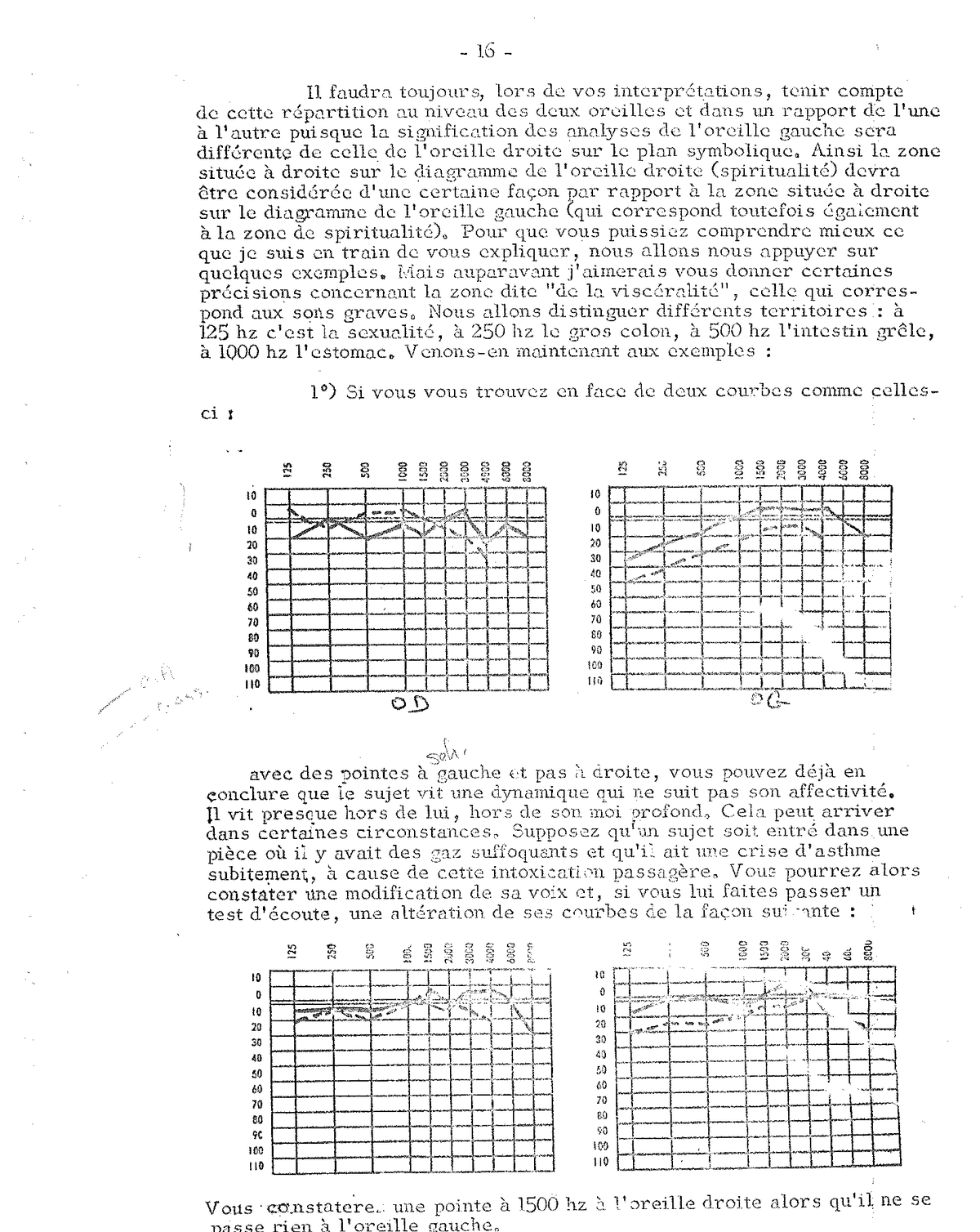
In your interpretations, you must always take account of this distribution at the level of both ears and in a relation of one to the other, since the signification of the analyses of the left ear will differ from that of the right ear on the symbolic plane. Thus the zone situated on the right on the right-ear diagram (spirituality) will have to be considered in a certain way in relation to the zone situated on the right on the left-ear diagram (which corresponds however also to the zone of spirituality). So that you may better understand what I am explaining to you, we shall lean on a few examples. But beforehand I should like to give you some clarification concerning the zone called “of viscerality”, the one corresponding to the low sounds. We shall distinguish different territories:
-
at 125 Hz, sexuality
-
at 250 Hz, the large colon
-
at 500 Hz, the small intestine
-
at 1,000 Hz, the stomach
Let us now come to the examples:
1°) If you find yourself before two curves with peaks on the left and not on the right, you may already conclude that the subject is living a dynamic that does not follow his affectivity. He lives almost outside himself, outside his deep self. This may occur in certain circumstances. Suppose a subject has entered a room where there were suffocating gases and has suddenly had an asthma attack because of this passing intoxication. You may then observe a modification of his voice and, if you have him take a listening test, an alteration of his curves: a peak at 1,500 Hz on the right ear while nothing happens on the left ear.
Example: peak at 1,500 Hz only on the right ear — passing asthma attack, without underlying affective blockage (below). Above, two reference curves.
By contrast, if I have a peak at 1,500 Hz on the LE and on the RE, I know it is an asthmatic state (or at least an allergic ground) on an affective blockage. There is a problem with the mother. Being unable to attack her, the subject will traumatise in himself what he has integrated as being the mother — here the respiratory tree. He may have a pulmonary asthma (suffocation) or laryngeal (dry cough, especially at night) or nasal (hay fever, rhinitis, and so on).
2°) I take another example. I observe a peak at 250 Hz on the right and on the left. It is therefore a disorder at the level of the colon in a subject who somatically lives (RE) a colitis of affective origin (LE).
Example: peaks at 250 Hz on the right and on the left — colitis of affective origin (LE) somatised on the right (RE).
If this peak at 250 Hz appears only on the LE diagram and not on the RE diagram, it means that there is an underlying colitis of affective origin (vulnerability at colon level) which is not at present manifested, since the peak is not present on the RE diagram, but which risks emerging at any moment.
If, by contrast, this peak at 250 Hz is felt only on the RE diagram, it simply means that the subject ate badly the day before, that he has stomach ache. He does not live this perturbation on the affective plane. It is not a deep reaction.
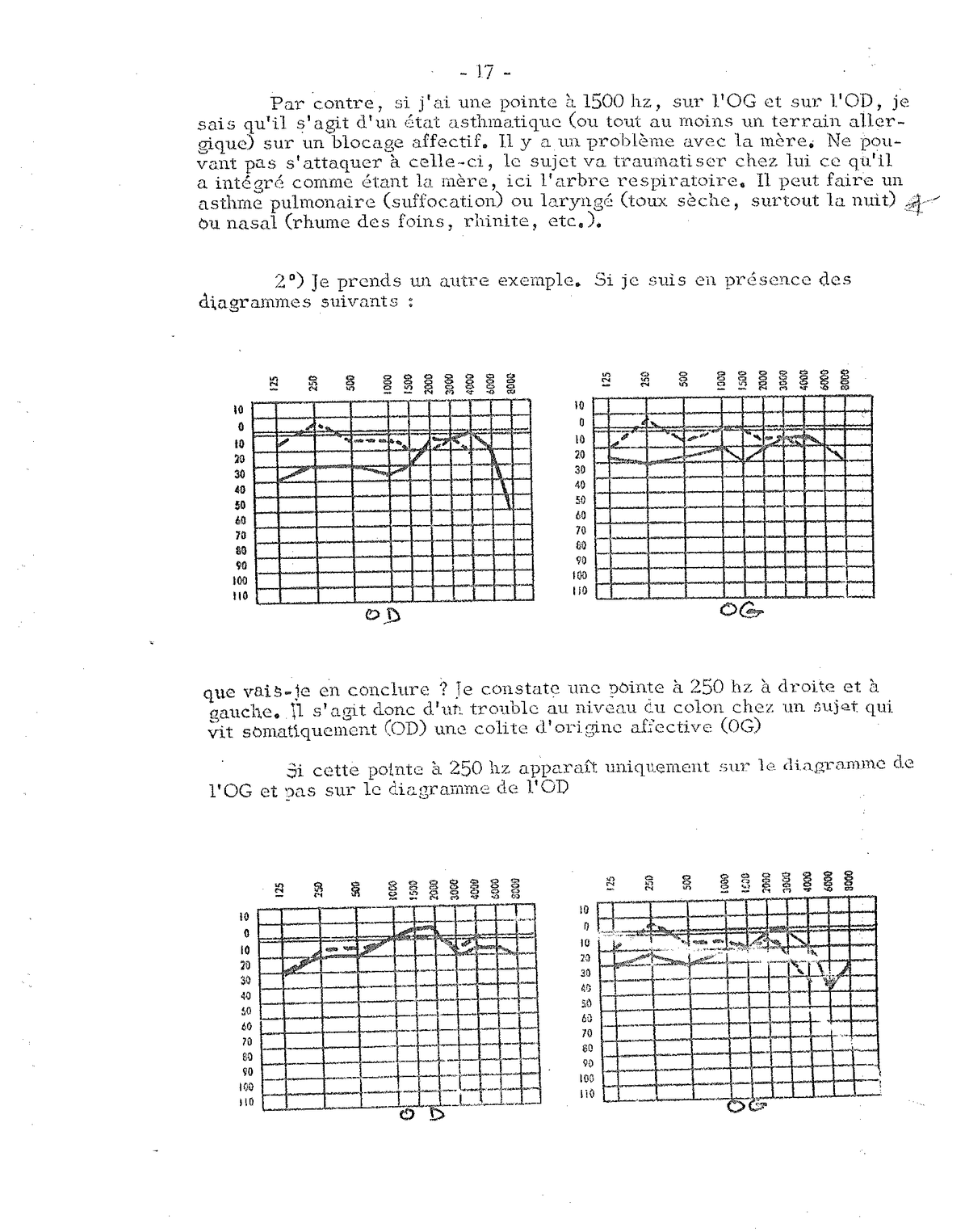
Peak at 500 Hz: small intestine disorder. According to whether the peak appears only on the RE (ate badly the day before), only on the LE (latent affective vulnerability) or on both (somatised affective suffering), the reading differs.
3°) As a third example, we take a curve with a peak at 500 Hz. I then know that the subject has a problem at the level of his small intestine. I can interpret these curves in the same way as before, according to whether the peak manifests itself on both diagrams at once, or only on that of the LE and that of the RE.
It is interesting to note that there is therefore a difference in reactions on the diagrams according to whether it is the large intestine or the small intestine. There even exists a notable difference on the vocal plane in terms of these perturbations. When one is well practised, one can know, just by hearing a subject’s voice, whether he suffers from his colon or his small intestine. This is normal, since they are different passbands on the audio-vocal plane. I had occasion to make, with gastroenterologist colleagues, experiments on the voices of their patients recorded on a magnetic tape. On listening to them, I was able to tell at what level the subject was suffering on the digestive plane, with almost no margin of error. I then thought that by modifying the subject’s voice, one could certainly improve his digestive state. But that is another matter on which I shall not dwell today. I continue to give you examples.
4°) If now you have a peak at 1,000 Hz, you find yourself in the presence of a disorder touching the stomach. In the same way, you will study the LE and RE diagrams to see whether it is an acute disorder (RE) or a chronic story (RE + LE) of affective order, or a vulnerability (LE) that risks manifesting itself at the slightest deficiency of the organism.
We have thus been able to make a tour of the so-called “visceral” zone, the body zone, the ego zone. When you have peaks in this region, it does not mean it is a visceral being, but it means he does not know how to rid himself of his organic universe, of the noises of his viscera, of the messages his ego intercedes as a signal. He sometimes hears his swallowing or his heart or his breathing; he thus lives a whole universe of anxiety that obliges him to remain too preoccupied with himself. Why would his heart not suddenly stop? Why is his breathing no longer the same? Why is his intestine making such a noise? His organic life takes on such importance that dialogue with the other passes to the background. It is moreover most often a question of persons who do not know how to listen to what is said to them, who speak about themselves permanently — of their pains, of their little ills. You see therefore that these indications are interesting. They make it possible to know the psycho-somatic state of the subject and to be informed of the inner sonic universe in which he lives.
One may of course analyse in the same way the following zone, which is that of language and lies between 1,000 and 2,000 Hz. You must examine what happens in this region on the right and on the left, look for whether there is a scotoma or whether, on the contrary, there exist peaks that may express an aggressiveness, more or less sustained, more or less expressed, according to whether the peak is situated on the LE only or on both ears. This is an important element on the plane of prognosis. You will indeed be able to indicate to the mother that, in the course of the audio-vocal education to which her child will be submitted, the latter will have such and such a reaction. If there is for example on the LE a peak at 1,500 Hz, I will be able to tell her that the reaction will be of the respiratory type. The child will start to suffocate or will give the impression of breathing poorly; sometimes even, an asthma attack (nasal, pharyngeal or pulmonary) is triggered. If the peak is at 250 Hz on the LE, you can indicate to the mother that her son suffers in his belly. You will see her little surprised at this affirmation, but on asking her, you will hear her say that her child has had diarrhoea or has been constipated for a few days. When I see a peak at 250 Hz, I cannot say what the digestive disorder is, but I can be sure that there is a problem at that level; I know that for this child his belly speaks to him; that is the language he expresses, and that is where there will be reactions during the treatment on the somatic plane.
Seventh question
And aggressiveness? How does it appear on the diagrams?
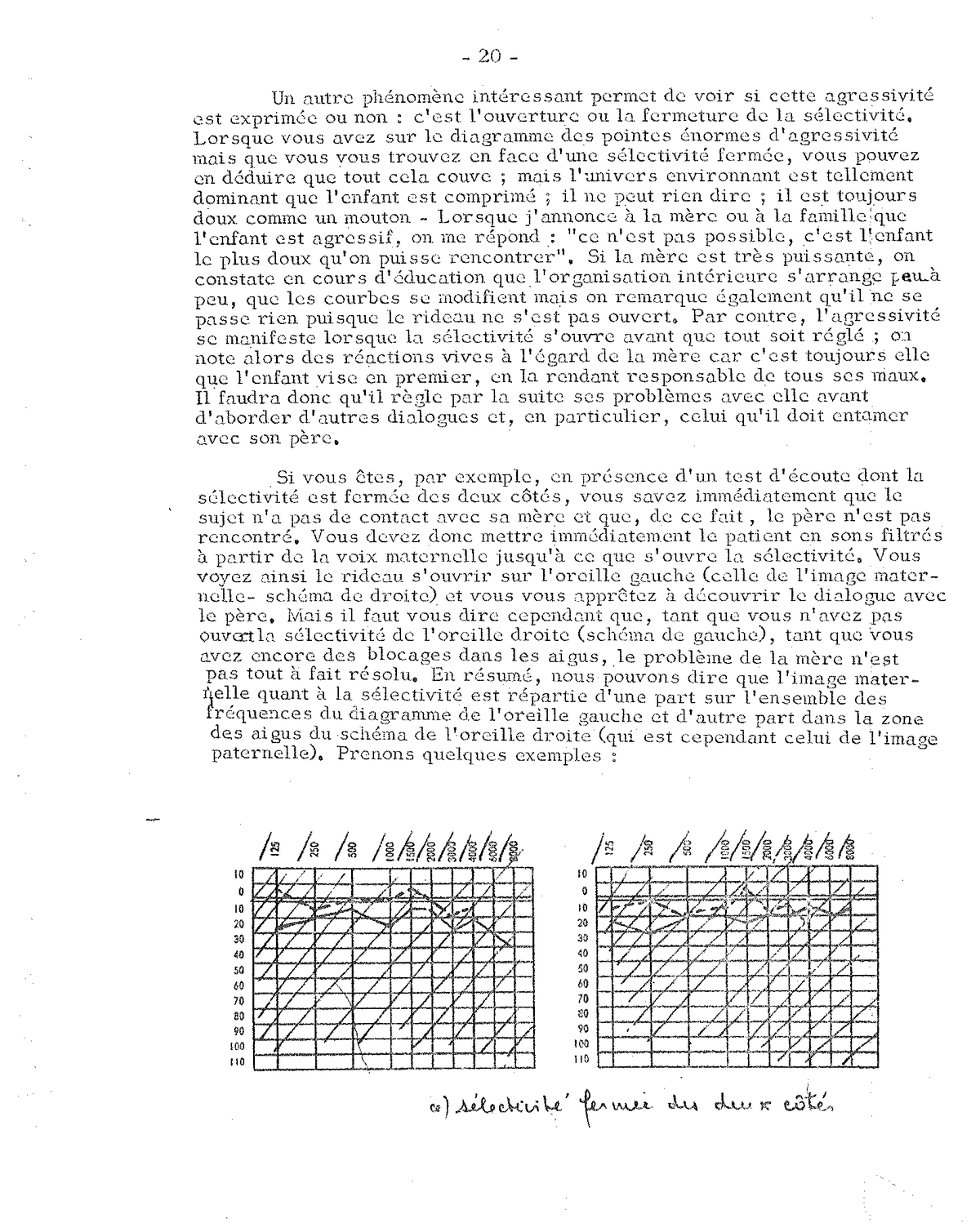
Professor Tomatis: Another interesting phenomenon makes it possible to see whether this aggressiveness is expressed or not: it is the opening or closing of selectivity. When you have on the diagram enormous peaks of aggressiveness but you find yourself before a closed selectivity, you can deduce that all this is brooding; but the surrounding environment is so dominant that the child is compressed; he can say nothing; he is always gentle as a lamb. When I announce to the mother or to the family that the child is aggressive, the answer is: “that is not possible, he is the gentlest child one could meet”. If the mother is very powerful, one observes during the education that all this gradually settles, that the curves modify themselves, but one also notes that nothing happens, since the curtain has not opened. By contrast, aggressiveness manifests itself when selectivity opens before everything is settled; one then notes lively reactions towards the mother, for it is always her that the child targets first, holding her responsible for all his ills. He will therefore have subsequently to settle his problems with her before broaching other dialogues, and in particular the one he must engage with his father.
If you are, for example, in the presence of a listening test whose selectivity is closed on both sides, you know immediately that the subject has no contact with his mother and that, by reason of this, the father is not encountered. You must therefore immediately put the patient in filtered sounds from the maternal voice until selectivity opens. You thus see the curtain open on the left ear (the one of the maternal image — diagram on the right), and you prepare to discover dialogue with the father. But you must however tell yourself that, as long as you have not opened the selectivity of the right ear (diagram on the left), as long as you still have blockages in the highs, the mother’s problem is not quite resolved. In summary, we can say that the maternal image regarding selectivity is distributed on the one hand on the whole of the frequencies of the left-ear diagram, and on the other in the high-frequency zone of the right-ear schema (which is however that of the paternal image).
a) Selectivity closed on both sides: no contact with the mother, the father is not encountered. Immediate indication of setting in filtered sounds from the maternal voice.
b) After 20 sessions of filtered Maternal Voice — c) After 40 sessions: the left ear has opened, but the right side of the right ear remains blocked from 4,000 Hz, sign that the maternal problem is not quite settled.
Eighth question
Could you explain to us why, during the study of selectivity, when a subject makes an error for example between 500 and 1,000 Hz, it is said that selectivity is completely blocked from this value on?
Professor Tomatis: Indeed, when there are deficiencies of analysis in a zone in the lows, there is a strong chance that the selective power of the highs is non-existent. I can affirm this to you from experience, but it is still difficult for me to tell you why. What is certain is that the subject cannot use the bands above the non-selective zone. The latter is a kind of barrier that confines the subject to the zone of the lows. One may moreover note that his voice is aggravated, that it lacks high harmonics.
In other words, whether there is total blockage of selectivity or only a blockage between 500 and 1,000 Hz for example, the result is the same. There will be no possibility of selective analysis in the zones situated above the blocked frequencies. It is certain that, on the re-educational plane, it will be easier and quicker to obtain an opening when there is only a partial closure. As soon as the barrier is removed between 500 and 1,000 Hz, to take the same example, all the other zones will then light up very quickly, and the subject will be able to benefit from all his underlying vitality, which was then in a state of sleep. While when selectivity is blocked over the whole of the frequencies, the work is longer. The uncultivated zones must be cleared little by little and given life.
It is with selectivity as with certain scotomas situated in the zone of the lows. These constitute the same barrier that prevents the individual from going beyond the “scotomised” zone. The subject will not use the sound range corresponding to the highs. He will always speak in a low voice; if he sings, he will have difficulty “rising” as one says in the trade. There again, you will be able to intervene rapidly, for as soon as the scotoma is filled, all the underlying possibilities will burst out in a brilliant sheaf, and you will then see the voice light up in a surprising way.
This phenomenon is more easily detectable for the sung voice than for the spoken voice. When you have a scotoma of 15 decibels at 500 Hz, the subject may have two voices when he sings. He can express himself perfectly in the lows then, at a given moment, he jumps over the scotoma and finds himself in another register. It has happened to me to see opera singers enter my surgery, come to consult me because suddenly they thought they were giving a G, and it was the high E that came out. This was due to a scotoma. I put them under Electronic Ear, and as soon as I was able to give them back control of quality (by suppressing the scotoma), they were able to start singing again without finding themselves before such phenomena, as surprising as they are disagreeable.
Ninth question
For the selectivity test, one realises that very often, children do not understand what is asked of them. One may explain to them what a low sound is and what a high sound is, but they reply indifferently, without perceiving the distinction. What is to be done then?
Professor Tomatis: One must first of all take up again the essential principles concerning this test. I notice that some of you like to please the patient by sending him several times sounds until he recognises a difference. In reality, you please yourselves, but you distort the test and you do not render service to the subject examined. The most important is that, at a given moment and in a fairly rapid way, the subject receives one piece of information, then another that he must situate in relation to the preceding. If he is wrong, that has no importance. You must only record it. It is certain that if you start again 30 times, he will end up no longer being wrong, but that is not what happens in life. When an individual receives a word and then another, he is in the obligation to analyse rapidly the verbal chain. There too, if you repeat the same word ten times, he will certainly end up understanding it, but this phenomenon does not intervene in the dynamic of the sentence.
As regards children, it is normal that the test is more difficult to administer than for an adult. But this is a question of pedagogy. The educator must learn to express himself so that the child understands what is asked of him. And if he does not understand the instructions, it is because, in life, he does not perceive either the subtle difference between one word and another. He does not know what “higher”, “lower” means, because he has no body image, because he is dyslateralised. His responses are characteristic of an impossibility of analysing the information that reaches him. In some centres dealing with the deficient, the educators sometimes complain of being unable to give the instructions. “They do not understand what is asked of them, what is high and what is low”, they say in speaking of the children they have to test. Then one day, in the course of a check-up assessment, they realise that the child perceives a difference between 500 and 125 Hz — it is because at that moment he begins to integrate what is asked of him, he begins to understand what is said to him.
You must therefore hold to the answers he gives you or does not give you in first analysis. The spoken chain is made of thousands of phonemes one must know how to distinguish so that the word reaches its true signification. The selectivity test is precisely made for one to recognise the auditory possibilities of the subject with regard to a pure tone, which is an enormous simplification compared to a word. A “pure” sound, as its name indicates, is a sound stripped of all ambiguity that should be easy to distinguish from another and to situate in relation to it. If therefore the individual cannot perform this selective operation between pure tones, how do you expect him to be able to distinguish the subtleties, the infinite variations, the multiple colours a word takes on within a sentence?
The human ear has exceptional possibilities of analysis. It can perceive at 1,000 hertz a difference of 3 hertz; it can also detect the direction of this variation, recognise whether it is a sound of 997 hertz or of 1,000 hertz, while situating them in the frequency scale. Consequently, it can easily distinguish the difference that exists from one octave to the next; there is indeed a world between the two pure tones sent into the subject’s ear.
Tenth question
We have until now spoken mostly of children. But we often encounter the same difficulties as regards adolescents and adults. They reply indifferently to the selectivity test “lower, higher, lower, higher” as if they did not wish to understand what is asked of them. Would there be other instructions to give?
Professor Tomatis: No. You must hold to what was taught to you for the administration of this test. And you must not, at all costs, make it so that the answers are good. It serves no purpose to start the test again on the pretext that the person has not understood what you ask of him. Some adults, in order not to appear stupid, to pretend to know how to distinguish one sound from another, reply anything in the test. In reality, they do not know how to discern the difference; they often confuse pitch and intensity; they have very few selective possibilities towards certain sounds, and particularly in the zone of the highs, which is the most subtle. But they do not wish to admit it. Leave them in their posture and record the errors.
What I have seen most astonishing in this kind of investigations are the responses collected from some musician singers or dancers. A tenor has different selective possibilities from those of a bass, just as a violinist walks in zones different from those of another instrumentalist for instance. As for dancers, they have in general a very poor ear. They hear practically nothing, on the selectivity plane, above 500-1,000 Hz. They perceive only the rhythms inherent in the body. Some become famous dancers precisely because they manage to cut the zone of melody. They are not great musicians; they are great rhythmics.
Eleventh question
By what test were you able to determine that children have a musical ear?
Professor Tomatis: Through counter-reaction at the voice level. Children all sing, they sing in tune, they immediately reproduce music. I mean of course normal children who have not had important affective traumas. I do not know whether you have already observed a child before a musical theme. He integrates it, he reproduces it by singing or by playing an instrument, he dances it, he mimes it, he lives it. He is music. It forms an integral part of his body. And that is why education through music, in particular in nursery school, is so important. One forgets a little too much at present this basic principle, because one wishes above all to intellectualise teaching; one wants to make of children beings full of knowledge. And it is then that the difficulties begin. Intelligence must mature slowly on a body ready to receive language.
The child at the outset has a musical ear, without distortions, without deformations. Our error is to wish to place too quickly on this still fragile nervous system knowledge, a semantics that will bring perturbations of a psychological order. Problems, complexes then arrive at great speed. The least vulnerable children are the deficient. Being unable to accede to the world of intelligence, they remain children sensitive to music, which they appreciate greatly, which they reproduce easily. The more gifted child will want to go further, will want to enter more quickly the linguistic universe that attracts him and towards which the grown-ups (parents and teachers) will try to draw him. And it is from this moment on that distortions appear. So as not to hear certain disagreeable things, certain voices, the child will scotomise, will truncate his auditory diaphragm, will distance himself from communication by choosing the longest circuits. He will then become an auditory left-hander, whereby he will lose all his possibilities of listening to language and of course to music. He will begin to sing out of tune, and as he will be made fun of, he will keep silent for a long time.
Twelfth question
The peaks of aggressiveness you spoke of just now, do they appear on the air curve or on the bone curve?
Professor Tomatis: Generally, it is on both curves that these asperities are encountered, but in some cases, there is compensation of the air curve in relation to the bone curve. One may very well, I repeat, die inwardly while giving the impression — at least for a certain time — of assuming the present. But this attitude of pomp ends up falling, and that is then the drama. One must beware of people who compensate, for one day, it is breakdown. One can thus foresee the latter by studying the subject’s curve, in the relations between the CO and the CA.
Thirteenth question
What information can a flat, straight curve give us?
Professor Tomatis: A straight curve does not permit analysis. This seems to indicate a non-differentiation from octave to octave. For the ear to be able to distinguish variations, there must be intervals, kinds of steps allowing the detection of the different pitches of sounds. On the physiological plane, one may try to explain this phenomenon as follows. The slightest low noise masks all the others. The inner ear is an apparatus that functions at constant pressure; it is a manometer, an accelerometer, so that as soon as there is a low frequency and, by reason of this, there is not enough tension to suppress it, this low frequency effaces all the others. It is here a phenomenon of masking.
The subject presenting a flat curve in reality only hears the lows and cannot analyse at the level of the highs. You will notice that such a curve is encountered in persons possessing a low, detimbred voice. It is found fairly often in the deficient, in subjects having few possibilities of analysis on the cortical plane. By the fact that they cannot use the high sounds to charge their cortex, one can understand, to a certain extent, their difficulties of integration, of comprehension.
The presence of an ascending slope is necessary for the ear to be able to block the low frequencies, to attenuate them, so that the proximal part of the cochlea may be used, more particularly in the zone devoted to language. This is specific to the human ear. The auditions of certain animals are, as regards passbands, much more developed than ours: the dolphin, for example, hears up to 200,000 hertz; certain bats and certain vampires, up to 150,000 hertz; a dog hears up to 45,000 hertz. But these are performances that represent little compared to the human ear’s faculty of hearing language. And this part of fine analysis requires that it not be hampered by the perception of low frequencies.
Why is this zone of language very important? Because it represents in fact the body image. If you try to make a table of frequencies, you observe that the lowest sounds (16 to 20 cycles) correspond to the lower part of the human body. And if you pursue this analysis in language, you observe that each wavelength touches, informs a part of the body, from the feet to the head, the low sounds corresponding to the lower part, and the high sounds (short waves) to the higher part. Distributed in this way, the frequencies of language are therefore adapted to the human body in order to be able to inform it in totality.
Is it language that has sculpted the human body? Or is it the latter that has obliged language to confine itself to frequency zones allowing the control of the body schema? I shall opt for the first hypothesis, recalling that man is a son of sound and liking to reflect often on one of the great sentences of Hermes Trismegistus: “It is sound that has fashioned the ear. And if you wish to know sound, learn first to study the ear.” In matters of language, men sculpt their body according to the sounds they emit. These sounds are moreover strongly influenced by the acoustic characteristics of the place. I often come to evoke the phenomenon of the American man of the United States. He is made of a very varied mixture of peoples coming from England, Germany, France, Italy, and so on, who all present rather marked linguistic distinctions. In the common acoustic atmosphere of the American continent, they all begin to nasalise (although the Italian and the Englishman in particular have no nasal in their language) like the Indian of the place. They take on the same psychomorphology as he; their face flattens, they become tall; in other words, they take on another body image according to the sounds they emit.
There is therefore a very important counter-reaction: language, body schema. That is why one can read on a listening test the integrated body image, from the feet (low frequencies) to the head (high frequencies).
Fourteenth question
Can you give us clarifications on this analysis of bodily posture in terms of the listening test, bringing in the spinal column?
Professor Tomatis: Yes. Posture itself undergoes auditory counter-reactions, through the play of the nerve bundles emanating from the utricles and saccules in the direction of the anterior roots of the spinal cord. It is by two routes that each motor root, holding under its sway the whole bodily musculature, finds itself cybernetically dependent on vestibular control.
These bundles I cite for memory, without wishing to weigh down this paper, are, I remind you, the homolateral vestibulo-spinal or Deitero-spinal bundles and the heterolateral vestibulo-spinals emerging from the Roller nucleus. Let us note here, in passing, a fact I believe essential and too often forgotten: the homolateral bundles, that is to say direct, hence non-decussated, are by far the most important. This is a capital point on the plane of laterality.
So, thanks to the vestibular circuits, a dynamic and static action will reflect itself on the overall posture of the column. To this function of permanent vestibulo-bodily subjection is added another, no less important, finding its source in the vestibular set which, issued from the same point, the Scarpa ganglion, radiates ascendingly towards the nuclei of the roof, of Schwalbe and of Bechterew. It is thanks to this latter set that the oculo-cephalogyric paths find themselves placed under vestibular sway. You therefore see the importance of it. I shall not dwell further on it, however noting that the 3rd, 4th and 5th pairs are linked together in their activities, on which the play of the 2nd cranial pair, that is to say the optic nerve, closely depends.
This bodily dynamic and statics are all the more vestibularly controlled and consequently reflected on our tests, since all the neurological elements to which we allude have their prothopathic sensory counter-reactions (that is to say in the domain of unconscious mechanisms) at the level of the archaic parts of the cerebellum, by the sensory bundles of Flesching and Gowers.
The corticalisation of this set, that is to say the awakening of the epicritic consciousness of this image unconsciously underlying and deliberately driven into mechanisms that sculpt its contours, appears with the cochlear system. The audiometric profile then takes on another dimension, that which we know of it, since this indispensable complement that is the cochlea is there to transform the analysis of the mechanical impulse received by the labyrinthine vesicle into acoustic-sonic activity. What the deaf person does not do, you will remember; he is incapable of carrying out this translation. Thus, thanks to the cortex in its recent part and to the push of the cerebellum of the same temporal level, these newly formed storeys evolve concomitantly with the neo-ear: the cochlea.
Any reading of the listening curve will therefore, for one who knows how to decipher it, reveal the mechanisms of psycho-somatic counter-reactions in some sense, through the musculo-bony play. There would certainly be a book to write on such a topic, but we shall content ourselves here with evoking the broad lines. Let us first recall that we may envisage several sorts of interpretations from the fact that each part of the body represents at its scale the whole body. There may therefore be as many developments as there are articles to detail. Let us take as an example the works of Nogier of Lyon, who developed auriculotherapy from the auricle of the ear. This physician, who discovered on the auricle a set of points corresponding to different locations of the body, has thus been able, thanks to acupuncture, to have a very precise action on the organism taken in its totality. It is the same for the cochlea, which has a metameric and segmental representation of the whole body.
We shall broach today the representation of the spinal column and that of the head. I shall join to it a rapid analysis of internal vagal activity, recalling to you that the vagus or pneumogastric nerve or 10th pair remains strongly bound up with tympanic tension, hence with listening. The curves will be read from the air tracing and the bone tracing. However, we shall dwell more on the bone curve for what concerns bodily bone conduction, which somehow marks an “interiority”.
Going from the lows towards the highs, we shall encounter the following points:
-
125 Hz: the pelvis and the feet — the genital organs
-
250 Hz: junction of pelvis and lumbar region — the colon — the knee
-
500 Hz: dorso-lumbar junction — the intestine — the elbow
-
1,000 Hz: the mid-dorsal region — the stomach
-
1,500 Hz: the dorso-cervical part — the lung
-
2,000 Hz: the cervico-occipital region
-
3,000 Hz: the skull in its upper part
There would certainly be reason to develop the reading of the whole pathology inherent in these phenomena, which reveal to us the psycho-somatic incidences of colitis, of affections of the small intestine or of attacks on the stomach of the ulcerative type, or eczema of the knee, of the elbow, or asthma — so many psychological fixations on the body, become in the circumstance the regulating valve of psychic dysregulations that cannot be dissolved and resolved in any other manner.
It would be interesting to envisage a new grid for the listening test taking account of these various considerations. To be able to study the position of the body in terms of frequencies, one might foresee a vertical and not horizontal reading. Man would thus be represented in his overall bodily attitude, so intimately linked to his psychic attitude. But this is only a projected idea that should be deepened so that each of us may propose a new diagram.
As for the position of the head, here too the bone curve taken as a whole reveals the posture of the cranial box in terms of the listening posture. If the lows are dominant up to 500 Hz for example, the frontal part is, consequently, higher than the occipital part. In other words, the plane passing through the culminating point of the forehead is higher than the vertex. By contrast, if the curve is ideal, ascending at 6 dB/octave, the vertex takes its place and becomes the culminating point, as its name designates.
Fifteenth question
Could you give us some clarifications on the organic deafnesses and on those of psychic origin?
Professor Tomatis: It is indeed necessary to scind well these two sorts of hypoacusis. It is certainly sometimes difficult to know whether it is really a listening difficulty due to an organic handicap or a refusal to hear of psychological origin. But given that one must not miss something serious, it is well to be prudent on the plane of diagnosis.
When you find yourself before a unilateral or bilateral deafness — that is, when you observe an important deficit, either on air conduction, or on bone conduction, or on both — you must at once think of having the subject’s ear verified by an ENT specialist, unless the patient has with him a report indicating the illnesses and interventions he has had in this field and that will justify the deafness.
I shall therefore examine with you schematically the different cases of auditory alteration of organic origin, which are grouped into three types of deafness:
-
conduction deafness
-
perception deafness
-
mixed deafness
a) Conduction deafness
It corresponds to a modification of the so-called “conduction” apparatus. It is usually agreed to group under this term all the elements that have the function of transmitting to the labyrinthine vesicle the sounds coming from outside. There is therefore reason to seek what obstacles may emerge on the path of sound which, taking account of the classical distribution, passes through the outer ear and the middle ear to reach the inner ear. Personally, I consider that there are only two blocks: the outer ear and the inner ear, the middle ear being the intermediate place between the mechanisms of the outer ear and those of the inner ear. The perturbation called “of conduction” will therefore intervene at the level of these two storeys.
The obstacles to be foreseen may be of several sorts and reach:
-
either the external auditory canal: wax plug, osteoma of the canal, external otitis with boils, eczema, and so on
-
or the eardrum, by thickening or loss of substance
-
or the tympanic cavity: otitis media, serous, sanguine or purulent, or even dry
-
or the ossicular chain: ostitis of the ossicles and especially fusion of the stirrup foot-plate (otospongiosis)
-
or the annexes: the Eustachian tube (tubular catarrh) and the mastoid cavities (mastoiditis)
Conduction deafness: the bone curve (dotted line) remains normal while the air curve (solid line) collapses in parallel. The CA/CO relation is inverted.
In the case of conduction deafness, the bone curve remains normal while the air curve collapses, remaining generally parallel to the bone curve. The CA/CO (air/bone) relation is therefore inverted. In other words, the organ of Corti is functioning well — which the bone conduction reveals — but the apparatus intended to transmit the sound to the inner stage is defective.
There is hardly any other solution but to remove the obstacle. It is for the otologist to intervene; it is to him that comes the primacy of the care which, from the simple removal of the wax plug, may go as far as the mobilisation of the stirrup. Deafness surgery is now very advanced and gives excellent results. You must therefore not hesitate, when you find yourself, for example, before otospongiosis, to direct the patient to a specialist capable of unblocking the ear.
It serves no purpose to try to re-educate an otospongiotic. You can however help him when the bone conduction begins to sag, so that the subsequent intervention may be more effective. You can above all be useful after the intervention — two to three months after — by allowing the freed ear to learn to listen, to analyse, to discern sounds it had no longer heard for years. I point out to you certain disorders that appear after the intervention, especially when the left ear has been operated on before the right ear. I recall to you that otospongiosis is an alteration of audition that is often bilateral. When the surgeon intervenes, he first operates on one ear, generally the most deficient, then a few weeks or months later, the other ear.
There is of course interest in having the right ear operated on first, which is, as you know, the most important on the plane of the controls of language, of memory, of concentration, and so on. But when, for a particular reason, the specialist begins with the left ear, you must support the patient by putting him under Electronic Ear while waiting for the liberation of the right ear. You will hear him tell you, after the intervention on his left ear, that he certainly hears better but that he has not entirely recovered his balance, or that he has migraines, or that he has memory gaps, or that he cannot manage to concentrate, or that he has several of these symptoms at once. Your role will consist in giving him an adapted programming, allowing him on the one hand to harmonise his left audition and on the other to support his right ear while waiting for it to be operated on. If, for one reason or another, the latter cannot be operated on — that is to say, if the patient must content himself with hearing principally with the left ear — you can also intervene under Electronic Ear, by regular cycles, by making especially his right ear work with filtered music and certain sibilants. For the texts, there will always be reason to set the balance at 10 or 7 so that the person perceives the phrases well and does not become discouraged.
Here therefore is what one may say briefly of conduction deafness and the means of treating it. It is certain that, in this eventuality, the otologist has his say. It is not a question for us of trespassing on his ground, on the contrary. In many cases, he alone is entitled to take charge of operations. However, it would be desirable that he too concern himself with the various extensions that may be given to the usual investigations. There exist, beyond his therapeutic arsenal, techniques that may help the patient, either before or after his own intervention, with a view to improving the power of listening. I often address otospongiotics to a great specialist of Béziers who operates in a remarkable way and obtains exceptional results. As soon as the patient’s audition is in a state of functioning, I can then, with a few sessions of auditory education, perfect the work on the listening plane, teaching the newly operated subject to aim at sounds, to analyse them in a certain way, somehow to converge, and to use his ear for the purposes of communication.
Our techniques can also be appreciable when it is a question of fitting an otospongiotic with a hearing aid. Apart from the intervention just spoken of, there exists indeed another means of helping the patient hear: it is the hearing aid. For some persons whose curves present enormous distortions, it is well to envisage a few series of Electronic Ear education sessions in order to harmonise the curves and possibly raise the thresholds. The subject is then much more easily fitted with a hearing aid, by the fact that the distortions have disappeared. Some prosthetists send us their clients so that they may benefit from our techniques before buying a device. This avoids seeing them come back, dissatisfied with their prosthesis and furious at not hearing well.
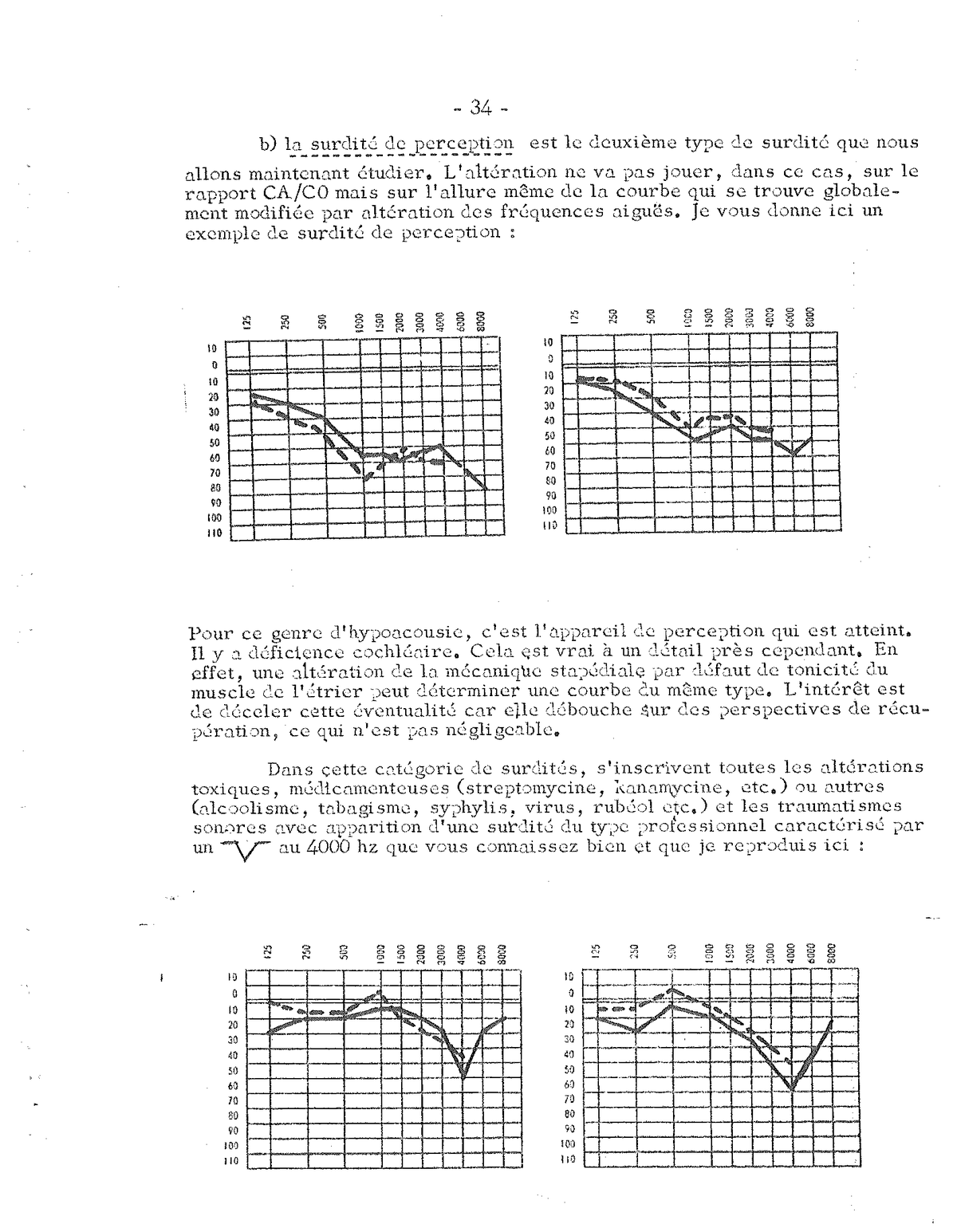
b) Perception deafness
is the second type of deafness we shall now study. The alteration will not play, in this case, on the CA/CO relation but on the very shape of the curve, which is globally modified by alteration of the high frequencies.
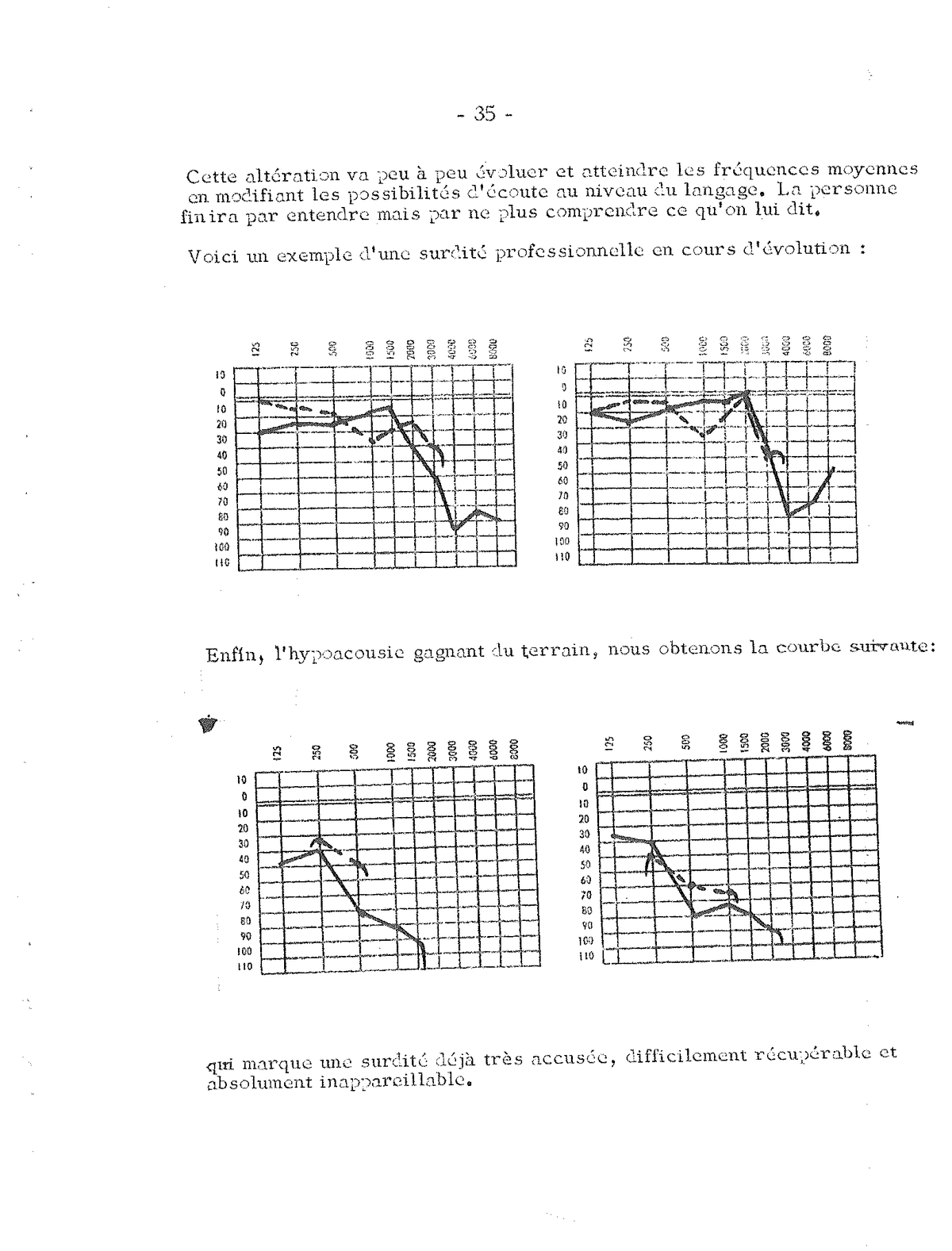
Above: perception deafness, global alteration of the curve by fall of the highs (cochlear deficiency). Below: occupational deafness characterised by a V at 4,000 Hz typical of exposure to sonic traumas.
For this kind of hypoacusis, it is the perception apparatus that is affected. There is cochlear deficiency. This is true with one detail however. Indeed, an alteration of stapedial mechanics by lack of tone of the stirrup muscle may determine a curve of the same type. The interest is to detect this eventuality, for it opens onto perspectives of recovery, which is not negligible.
In this category of deafnesses are inscribed all the toxic alterations, medicinal (streptomycin, kanamycin, and so on) or other (alcoholism, smoking, syphilis, viruses, rubella, and so on) and sonic traumas with the appearance of a deafness of the occupational type characterised by a V at 4,000 Hz, which you know well. This alteration will gradually evolve and reach the middle frequencies, by modifying the listening possibilities at the level of language. The person will end up hearing but no longer understanding what is said to him.
c) Mixed deafness
represents the third category of deafness. As its name indicates, it belongs to the type that associates the two preceding anomalies — that is to say, it is an interlocking of one and the other of these two processes of otological pathology. Its characteristics indeed reveal disorders of the conduction mechanisms joined to alterations of the perception phenomena. The bringing together of these two perturbations easy to trace is read on the graph by an inversion of the air-bone curve — as we have described in the study of conduction deafness — and by the fall of the highs on both the CA and CO curves, the latter of course remaining parallel as conduction deafness requires.
Occupational deafness in evolution (above) and then deafness already very pronounced (below) — becomes difficult to recover and to fit a hearing aid to.
Mixed deafness: interlocking of a conduction deafness (CA/CO inversion) and a perception deafness (fall of the highs on both curves, which remain parallel).
Thus we have been able to broach the study of so-called organic-origin deafnesses. I have given you in the circumstance only the principal keys allowing one to detect, in their broad lines, the essential traits that must draw the educator’s attention so that he may direct to the otologist specialist such anomalies as are not within his competence. You should however know that, in some cases, it is possible to have our techniques act, but only great practice can help to make differential diagnoses concerning these anomalies.
An attempt at auditory education under Electronic Ear for a few sessions — about twenty — may however constitute one of the best means of eliminating the causes of error. Through the rapid modifications that may occur on the two curves or on one of them, one can know whether the organic origin is determining or not. Thus, for some non-otospongiosis-characteristic conduction deafnesses, it happens that the curves “move”, which proves that the ossicular chain may still be mobilisable by re-educational means. This fact is often observed in children, in whom cases of otospongiosis are moreover very rare. It is then possible to think of a deafness of psychic origin, of a refusal of listening that then yields to the psycho-sensory approach one can carry out under Electronic Ear with the help of an adapted programming. By contrast, if the ossification process has passed the limits, it will be impossible for you to intervene on air conduction, which will remain fixed, while bone conduction, as I told you just now, may sometimes improve perceptibly, thus allowing a greater efficacy of the means to be envisaged — surgery or prosthesis.
Before broaching with you the other deafnesses, those of psychological origin, I should like to say a few words on the associated disorders that accompany these different kinds of deafness: headaches, tinnitus, vertigo, nausea, and so on. In all cases, you can relieve the patient, which is already much. A well-conducted education must make these various disorders disappear, 9 times out of 10, by re-equilibration of the whole vestibular apparatus and toning of the eardrum.
Psychological deafnesses
Let us now come to psychological deafnesses. “None is more deaf than the one who does not wish to hear.” You all know this leitmotif, and you all live it every day by re-educating children and adults who have deliberately decided to listen no more, who have cut communication with the environment. I recall to you that a human being has at his disposal several means of disconnecting his listening. You can observe this by studying the diagrams corresponding to this policy of non-communication. Here are a few main lines:
a) The subject can first of all lower the thresholds of his audition so as no longer to hear very distinctly. You are then in the presence of a hypoacusis, slight or already pronounced, bearing on both ears or on one of them. The fact that it is the left ear or the right ear already gives you indications on the affective problem of parental origin that is at the basis of this hypoacusis.
b) The individual has decided to close the curtains so as no longer to see what is happening outside. Selectivity is blocked either over the whole of the frequencies on the right and on the left, or only on a part of the sound scale for both ears or for one of them. We have broached this question a few moments ago in evoking the problem of selectivity.
c) A third “trick” consists in blurring the cards, in no longer knowing where the sound comes from, in living in confusion. It is the brouhaha characterising the disorders of spatialisation that form the object of the third test concerning the listening test.
d) Finally, there is the possibility of putting the other at a distance by choosing the longest circuits — that is to say, by taking the path of the auditory left. You then see, on the audio-laterometer, the left audio-vocal circuit becoming dominant.
Here therefore is what we can say today, within the framework of this Congress, on the different deafnesses arising from an organic or psychic origin. It is plain that we have only been able to evoke a few broad lines. It would be necessary to deepen subsequently these questions in the course of certain meetings that would permit the carrying out of well-defined case studies.
Sixteenth question
What is to be done for a person who, after an operation, still hears an accordion?
Professor Tomatis: It would first be necessary to specify whether the internal noises she hears are really characteristic of music played by an accordionist, in which case we shall be able to think of a phantasm, of a sound hallucination, or whether they are tinnitus that perhaps vaguely recalls a sound of an accordion but that approaches above all the buzzing or whistling of the ear usually encountered in some cases of deafness.
It happens that the intervention, although re-establishing auditory function, does not completely suppress the associated disorders that present listening difficulties. We must not let this chance pass and we must do everything so that these various symptoms disappear. You have no doubt often encountered, through your activity, persons who suffer from tinnitus and vertigo, and you know the hell in which these patients live. It is absolutely frightening to hear internal noises permanently and to live in a constant vertiginous state.
If we retain the other hypothesis, that of sound hallucinations, we must of course take another attitude and pursue the investigations on the psychological plane. A psycho-sensory approach under Electronic Ear may also be very effective by giving the individual the desire and the possibility of communicating with the outside world, of dialoguing with his environment, of thinking of others rather than shutting himself in an egotic attitude that earns him a few rather unexpected interpretations.
This question reminds me of an experimentation done at Sainte-Anne some fifteen years ago. I had asked to examine hallucinated patients in order to know their auditory faculties. It was then that I had the surprise of observing that these mentally ill patients had in reality two audition thresholds. The first, very subtle, very fine, brought such replies as “there, that’s it, I recognise the voice that speaks to me every evening, that tells me this, that tells me that”. Then, by insisting in order to reach a more intense threshold, I obtained reflections such as “Ah! there, I hear noise”, with a few commentaries of the kind “it is bright” or “it is dark” or “it is blue” or “it is red” or “it is greasy”, and so on.
There are therefore for these patients two sorts of auditory reference that moreover exist in everyone, but which we shall not interpret in the same way. The first threshold, so subtle, so tenuous, is that of the molecular noise, of the Brownian movement that one can reach by putting oneself into the listening posture. It is the one that recharges us, that is necessary to us to reach certain zones of thought, but that is not imperative with us. The second, more heavy, more material, is situated at a lower level and rejoins the common preoccupations of the sonic world.
I learned much by living with and re-educating some of them. Their various reflections on what they were hearing enabled me to make great strides in research. When they told me: “It is the sound of a bell”, “it is the village bell ringing”, “it is the sound of the sea”, “it is the sound of waves” … I thought that they were right and that they perceived things our ratio no longer allowed us to hear. I was thus able to dialogue with them on a plane wholly different from that usually encountered in the conversational universe, and I was able, again thanks to our techniques, to lower their thresholds so that they might set themselves at the level of the common of mortals. When the reconnection was made, alienation of course disappeared, since the references became the same. I have got several of them out of hospital…
The problem of sound interpretations from a noise and sometimes from a pure tone made me then think of a test of which I spoke some years ago in one of my lectures and which a Swiss psychologist was able to carry out and publish (I can give you the bibliographical reference if you wish). It was a question of making a kind of sound Rorschach from certain noises determined in advance and of noting the various interpretations. The results were very revealing of the individuals’ psychic universe. It has certainly happened to you to ask yourself what is happening when you hear a noise in the night, and you have certainly given yourself a good fright, when it was only a door slamming or a beam creaking.
I therefore think that there is a great work to be done in this direction, and I invite you all to think of this sound test, which may give extraordinary indications on the inner world of the patients in our care. All your suggestions will be welcome, so that we may develop a complete battery making possible the establishment of statistics from the results obtained in each Centre.
Seventeenth question
What is to be thought when one finds oneself before a subject who has an excellent right ear but who, on the other hand, has a deficient left ear whose air curve begins to descend from 3,000 Hz down to 60 decibels and whose bone curve lies above, zig-zagging?
Professor Tomatis: If beforehand you have eliminated the hypothesis of an organic story (former otitis with paracentesis, trauma of the ear, and so on), you must of course think of a psychological origin.
The first reaction might be this: “It is the left ear, it is therefore not serious, since the right ear is intact”. We all know that the right ear is essential in all the control processes, but that does not mean that the left ear has no importance. There must always be, I repeat, harmonisation between left and right. It is therefore the problem of laterality that emerges again, with its symbols and its multiple implications.
Since it is the left ear, you must think at once of a maternal relation problem. There is hooking to the mother, so that dynamics, becoming, the father whom the right represents, remain still a myth. There is a blockage; there is fatigue. As soon as the individual wishes to go forward, to make projects, to launch himself into a new business, he is stopped, he is held back. He begins everything; he finishes nothing. It is the policy of failure. He remains shut in his maternal problem, and as long as he has not resolved it, he will not be able to go further.
When I say that there is blockage at the level of the mother, this means an internal relational problem, a matter of the ego, of the self, of the unconscious with respect to the transcendental “I”, to the “I” of the “Verily, verily, I say unto you” of full consciousness. There, we walk in the “I cannot advance, I am tired, I this, I that”. They are the blades of the unconscious that point through. It is the unconscious that expresses itself and not consciousness. As soon as the latter appears, the two curves take on the shape you know well and that we have discussed on several occasions during these working days.
What is to be done then before such a case? The importance of the maternal problem requires of course that one undertake in the first place an education in intra-uterine audition from the mother’s voice. The sonic births must follow this foetal period and be distributed in a fairly intensive way so that the subject may at last unhook himself from the maternal core. The following phase must not consist in trying to make the left ear “rise” by keeping the balance at 7 (cord on the right) or by placing the cord on the left with the balance at 1. One must, on the contrary, rapidly lateralise to the right, and you will then have the surprise of seeing that the left ear improves perceptibly. Indeed, it is necessary to think that there exist enormous bi-auricular counter-reactions, notably through bulbo-protuberant junctions, like the Rasmussen bundle that throws a bridge between the two cochleas.
Eighteenth question
I think I understood that the child loses very quickly after his birth a part of the perception of the highs. Is that the reason why the father’s voice is filtered in a fairly low zone, between 300 and 800 hertz, I believe?
Professor Tomatis: The diaphragmatic opening of the child’s audition takes place in a very progressive way. It is true that at his birth, from the 10th day more exactly — that is, from the moment when the Eustachian tube abandons its fluid — the child finds himself plunged into a sonic “black” that no longer allows him to hear the high frequencies he perceived perfectly during his foetal life. He does not yet know how to pull on his musculature in an aerial medium in order to recover his perception of the great highs, and his ear will have to perform for years a work of accommodation, of convergence in order to find again the high spheres of communication. We shall have to wait the age of 4-5 for the child to be able to pronounce sibilants very properly.
As regards the encounter with the father in an approach that will not yet correspond to the true dialogue the child will begin much later, we take account of this progressive opening and we filter the paternal voice so that it appears first in a band going from 300 to 800 Hz, then from 300 to 2,000 Hz, then from 300 to 4,000 Hz; finally we open the curtain totally when the preceding stages have not provoked dazzling or lively reactions in the child.
I recall to you that this period of encounter with the paternal voice marks a very important stage on the path of the realisation of the being. If the maternal problem is wholly resolved and if, after a linguistic preparation carried out with the help of a skilfully established programming, the dialogue with the father may institute itself, the game is won. The being, launched into an exceptional dynamic of life, will be able to assume all the difficulties of existence with surprising strength.
But we all know that things do not always go so well and that this famous “paternal” stage is one of the most difficult to cross. It must be broached by the educator in a very prudent way so that the confrontation is not dramatic and does not entail phenomena of regression, of inner retreat that will make us lose time. I think moreover that the first approach should be done in paternal voice filtered at 8,000 Hz, at this high altitude where problems are resolved on another plane. But this is only a hypothesis I shall speak of again as soon as we have experimented with it.
Nineteenth question
Since the child loses his highs at birth and only hears the lows, how is it that he has a high-pitched voice and sometimes even a very high-pitched one?
Professor Tomatis: A high-pitched voice must not be confused with a frail, pointed, tenuous voice. The child in reality has a “small” voice inscribed in a narrow band. There are few harmonics in a child’s voice. You note this moreover when you hear certain little singers try to “rise” in the highs. Their high notes are sometimes a little stiff and lack that bushy, rich harmonic sheaf one encounters in some adults.
The voice of the small child is mono-harmonic or mono-band. It reveals a still narrow auditory diaphragmatic opening, resembling moreover that of the haute-contres who are, as you no doubt know, singers able to “rise” very high in the scale. I knew one of them who had a very exceptional voice, and when I heard him, I thought he was going to blow up all my cathode-ray tubes during the analysis of his voice. Now, he did not exceed 1,500 hertz. He sang Mozart divinely, but he did so in a narrow band, which was that of his register.
Twentieth question
What happens when one administers a listening test to a subject who holds himself as he should to hear the highs? Are the responses different according to the patient’s posture?
Professor Tomatis: Yes, certainly, but when you administer a listening test to an individual, it is to know his posture in current life, which is most often an attitude of non-listening. It is plain that his responses will be different if you ask him to hold himself well straight, to place his head in a certain way corresponding to the fine perception of the highs, and so on. But given that this is not his usual attitude, this procedure will only have the value of an experiment.
You yourselves have certainly noticed, during a concert for example, how different music is if you listen to it in “high-frequency posture” or if you slump in your chair. We then find again the comments we made recently about the place of the head in the listening test. The perception of the highs determines a certain tracing, while the perception of the lows determines another. The first, corresponding to the maximum tension of the stirrup muscle, is found in the experiments done by the Americans, Möller, Schmitt and Reger, with a curve of 12 dB/octave, while the second calls on a relaxation of the stapedial musculature and plunges the being into the depressive universe of the low sounds.
The ideal, of course, is to be constantly in the posture of listening to the high sounds. This presupposes a putting into condition that requires a certain training. I have just evoked the work carried out by a team of researchers who have ended up demonstrating that one can condition the human ears to hear in several ways, which in fact I have been striving to say for 25 years. They found that, by pulling on the muscles of the hammer and the stirrup, they could determine a slope of at least 15 decibels between 250 and 1,000 Hz.
This tension of the muscles of the middle ear must therefore be sought permanently and in any circumstance. If you are plunged in a disagreeable, disharmonic sonic universe rich in low frequencies, or if you are obliged to hear things of no interest or said in an aggressive way, you must manage to put yourself in the posture of listening to the highs in order to recharge yourself and to benefit from the maximum of the sound environment while avoiding the negative side. Personally, I always do this on an aeroplane in order to arrive fresh and rested at the place where I most often have to consult immediately or give a lecture. I always manage to put myself in the posture of listening to the highs during the trip, while I see beside me people slumped, annihilated by the low frequencies and the vibrations the device transmits.
Why are low sounds so dangerous? Because they require of the body more energetic expense than the cortex receives stimulation. Sounds such as those of the tom-tom for instance have precisely as their aim to make the body move and to place the individual subjected to this second state in a kind of hypnosis that places him at the mercy of the sorcerer. While the high sounds, such as those found in Gregorian chants, recharge the subject, lead him towards consciousness, without however drawing him into a mobile bodily image. Let us end by speaking of military chants, which combine the two procedures: they recharge the subjects while making them march as a single man.
Twenty-first question
Is there a curve characteristic of the depressive?
Professor Tomatis: Yes, just as there exists a curve characteristic of the paranoiac, of the claimant, and so on. That of the depressive has this general shape of a curve descending from the lows towards the highs, which is the inverse of the recharge curve. Several eventualities may of course present themselves according to whether the individual compensates or does not compensate his depressive state. You may then have the following schema, in which you observe the depressive state at the level of the bone curve. By contrast, the air curve gives the change and allows the subject to hold up apparently.
Depression and fatigue must not be confused. Often an individual comes to see you because he feels depressed. In fact, he is exhausted and no longer knows how to recharge himself. You then find yourself in the presence of a tracing where the bone curve is not falling.
As a general rule, you can conclude in the presence of a depressive state when you see the bone curve descending from the lows towards the highs.
Twenty-second question
What is the support that can make the unity of all this? Is it a neuronic support or a psychological one?
Professor Tomatis: Given the plane on which such a question risks placing us, it would be somewhat illusory to wish to answer it without at least committing oneself to a philosopho-psycho-physiological diatribe without issue. One remembers the endless dialogue that opposed Aristotle to Anaxagoras regarding the prevalence of the brain and the hand. Which of the two organs allowed man to be what he is? No one can answer it.
It is the same as concerns us. In the perspective in which the question posed places us, the psyche is as necessary as the nervous system, its instrument, as the violin is necessary to the violinist. The one needs the other to respond to a higher instance, which is music in this instance. For us, it is the call to transcendence that fixes our attention around listening, drawing man towards his conscious field.
Promoted somehow by a complex neuronic organisation he cannot escape, the human being thus finds himself having to respond, at his scale, to motivations that will manifest themselves in him by a desire to communicate, to understand, to know. In fact, these motivations will be only injections coming from one knows not where, true incursions of consciousness acting as the first manifestation of the life that animates the being.
Conclusion
This succession of questions could be prolonged to infinity, so immense is the field of investigation concerning the listening test. So it appears useless, after this first study, to insist on the value of such a test, which takes on considerable importance.
Much certainly remains to be done, and Professor Tomatis is profoundly conscious of it. If we wished to gather the information he kindly transmitted to us on the occasion of our 3rd International Congress, it is because we also consider the interpretation of the listening test as essential.
This research, so rich in teaching for audio-psycho-phonology, must be patiently taken up, broadened, supported by wide practice, so that the works undertaken in this direction have an effective extension in the field of diagnosis and therapy.
Numerous subsequent meetings focused on the same topic and based on very varied case studies will make it possible to elaborate, in the years to come, a complete work on the interpretation of the listening test, the interest of which will not escape any of those who deal with the problems of the relation of the human being with his environment.
Source: A. A. Tomatis, “Considérations sur le test d’écoute”, printing published by the Société d’Audio-Psycho-Phonologie, 4 rue Cozette - 80000 Amiens, June 1974, forty-eight pages. Remarks gathered at the 3rd International Congress of Audio-Psycho-Phonology (Antwerp 1973). Document digitised from the personal archives of Christophe Besson.