The Nuisances of Noise
The Nuisances of Noise — Occupational Deafness, Plant Audiometry, Objective Audiometry (Le Médecin d'Usine, 1957)
Synthesis written by Alfred Tomatis for the journal LE MÉDECIN D’USINE (November 1957, pp. 605-624). The author here brings together, for the attention of occupational physicians, his research on occupational deafness — installation, latency, sub-total latency, manifest deafness —, on plant audiometry, and on objective audiometry by phonation-audition feedback, the first results of which had been published at the same period in the Journal Français d’Oto-Rhino-Laryngologie (May-June 1957). There figure, in a form accessible to factory practitioners, the concepts of directing ear, of auditory and vocal scotomata, and of racial auditions (Italian, French, Russian), as well as twenty-two figures (audiograms, diagrams of transcerebral transfer and of the electronic mounting).
NOISE
The nuisances of noise
By Dr Alfred TOMATIS (Paris)
Occupational deafness — Plant audiometry — Objective audiometry
Printed with the periodical LE MÉDECIN D’USINE, November 1957, pages 605-624.
I. — Occupational deafness
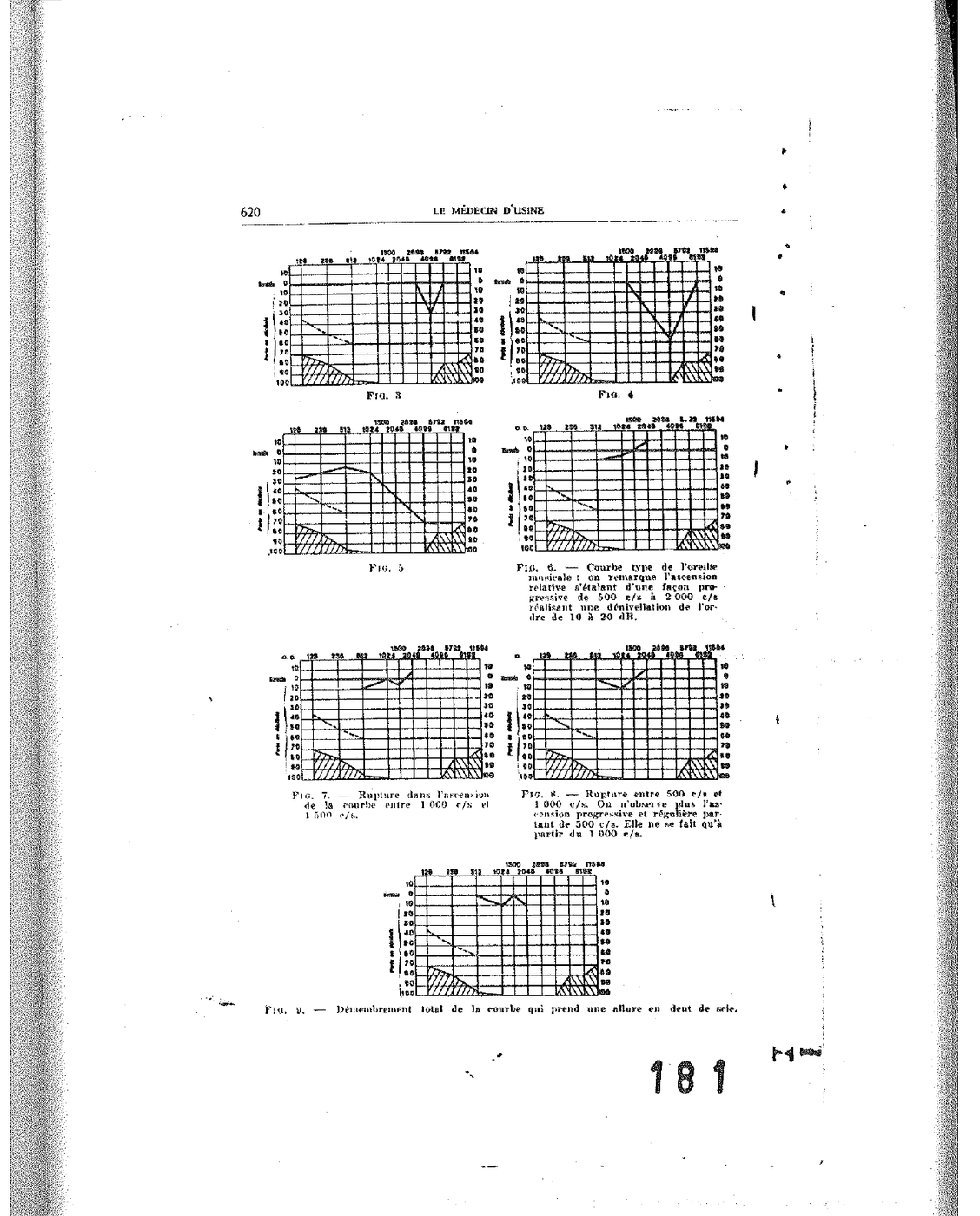
Any auditory deficiency of occupational character presents itself, from the beginning, under the aspect of a lesional mode of typical appearance: constant, elective audiometric fall on the frequencies neighbouring 4,000 cycles per second, and in particular on the 4,096 c/s frequency. A carefully conducted audiometric examination brings out four successive periods:
1° Period of installation of the permanent deficit. Very precocious, it is translated, from the first hours of exposure to noise, into a fall of audition bearing exclusively on the high frequencies, around 4,000 cycles. This fall is reversible if the subject is withdrawn from the noise; it will no longer be reversible after several weeks or several months of continuous exposure. The deficit, now permanent, is very limited — it bears on two or three frequencies only — and the subject has no awareness of the discomfort that affects him. Conversation unfolds normally, and only an audiogram carefully conducted allows the demonstration of the lesion which is beginning.
2° Period of total latency. The deficit remains limited to the high frequencies, but slowly enlarges. The subject continues to experience no subjective trouble. This period, which can last several years, is the most dangerous: it unfolds without the subject’s knowledge, and without the knowledge of the physician himself who has not requested the audiogram.
3° Period of sub-total latency. The deficit, by worsening, progressively reaches the neighbouring frequencies: it first gains the high sounds neighbouring 4,000 cycles, then descends slowly towards the median frequencies. A few subjective troubles appear: sensation of strangeness of certain consonants — sibilants, fricatives — and difficulty of comprehension in ambient noise. Conversation remains possible, but listening to the telephone, or the perception of the voice of an interlocutor situated at some distance, becomes painful.
4° Period of manifest deafness. The deficit, now extended to all the conversational frequencies, becomes subjectively objective and the subject consults. The deafness is manifest, irreversible, and any protective measure arrives too late. The role of the plant physician is precisely to avoid arriving at this stage.
[Figs. 1 to 4 — Type audiograms of the four successive periods of occupational deafness.]
II. — Audiometry
Audiometry has as its object the quantitative and qualitative measurement of auditory thresholds across the whole spectrum of audible frequencies. It is practised with an audiometer — an electronic apparatus delivering pure tones of variable intensity, calibrated in decibels with respect to a normal reference audiogram — and is translated into a tracing: the audiogram, on which the frequencies are placed on the abscissae (from 125 to 8,000 c/s) and the auditory losses in decibels on the ordinates.
Threshold tonal audiometry is the most widely employed method: it measures the minimum threshold of perception of the pure sound. It is usefully supplemented, in certain cases, by suprathreshold audiometry (Fowler trials, S.I.S.I., recruitment) and by vocal audiometry, which measures the comprehension of speech.
III. — Plant audiometry
Plant audiometry differs from office audiometry by three requirements:
1° Rapidity. The plant physician must be able to effect, in a few minutes, the examination of a great number of subjects. The threshold examination bearing on the essential frequencies — 500, 1,000, 2,000, 4,000 and 6,000 cycles — suffices to detect the beginning lesion.
2° Reproducibility. The conditions of examination must be rigorously identical from one examination to another, in order that the variations observed be significant. This reproducibility requires a soundproof cabin — or at the very least a room sufficiently isolated from ambient noise — and a regularly calibrated audiometer.
3° Follow-up. Every exposed worker must be the subject of an audiogram on hiring, then of periodic audiograms (every six months or every year according to the degree of exposure), recorded on an individual file allowing the comparison of successive tracings.
The role of the plant physician is essentially preventive: detecting the beginning lesion at the stage when it is still reversible, or at the least limited, and having the necessary protective measures taken (cabins, helmets, earplugs, rotation of personnel) before manifest deafness installs itself.
[Figs. 5 to 9 — Characteristic audiograms gathered in industrial settings.]
IV. — Objective audiometry
Classical audiometry rests entirely on the sincerity of the examined subject. Now experience shows that this sincerity is lacking in many circumstances: subjects claiming to be afflicted in view of compensation, subjects concealing their deficit in view of hiring, subjects in good faith but incapable of judging correctly their own threshold. Objective audiometry proposes precisely to measure the auditory threshold independently of any cooperation from the subject and, thereby, independently of any simulation.
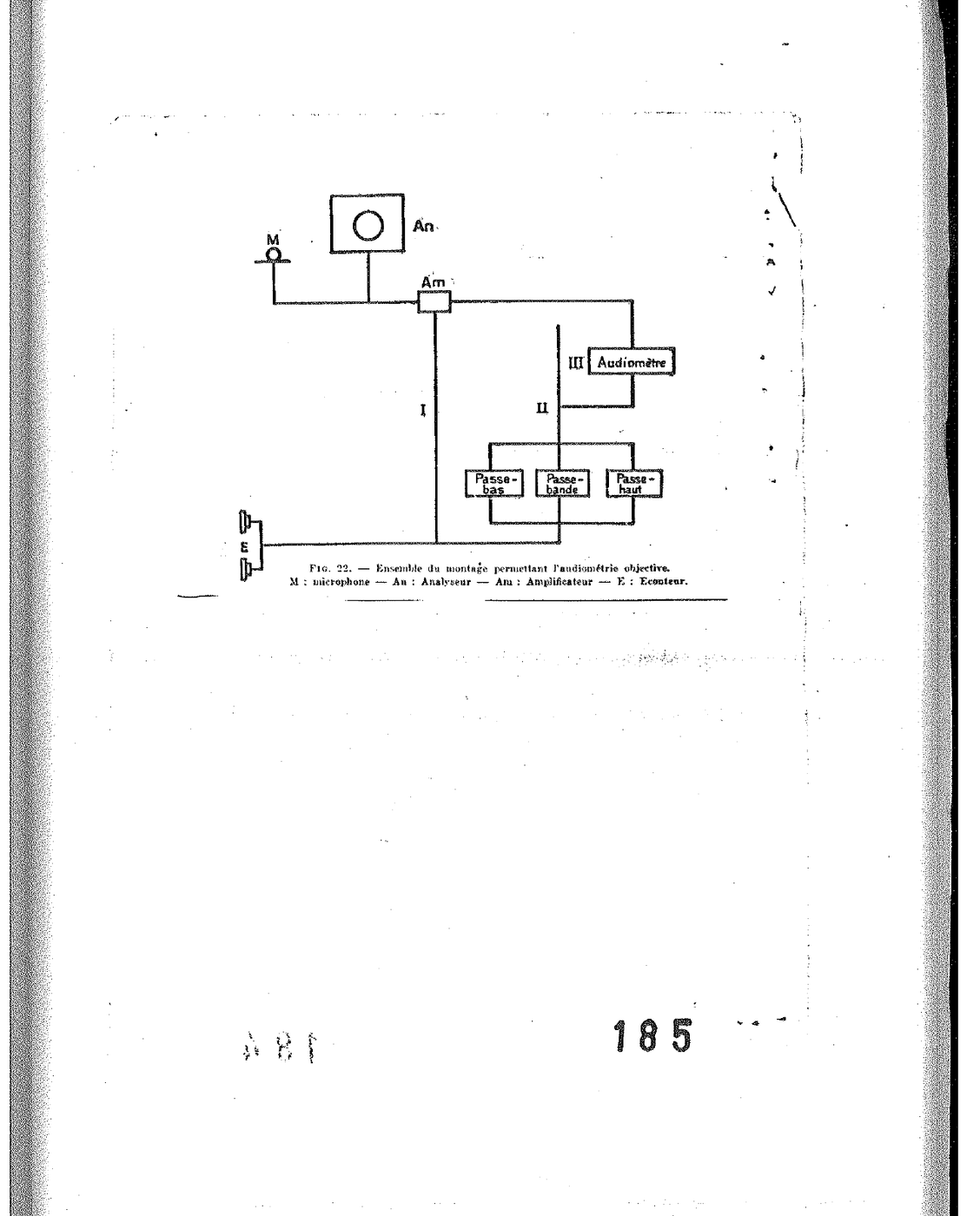
The principle is simple. Given the existence — experimentally demonstrated and published by us as early as 1954 — of a permanent counter-reaction loop linking audition to phonation, it suffices, to measure the manner in which a subject hears, to analyse the spectrum of the voice he emits. If one practises on the audition of this subject any modification whatsoever — for example a filtering that suppresses the frequencies above 2,000 c/s —, one observes instantaneously, in the spectral analysis of his voice, the disappearance of the same frequencies. The audio-phonatory counter-reactions, baptised “Tomatis effect” by Mr Raoul Husson in a communication of 4 June 1957 to the Académie Nationale de Médecine, thus furnish the means for a truly objective audiometry.
I. — Rhythm disorders: the directing ear
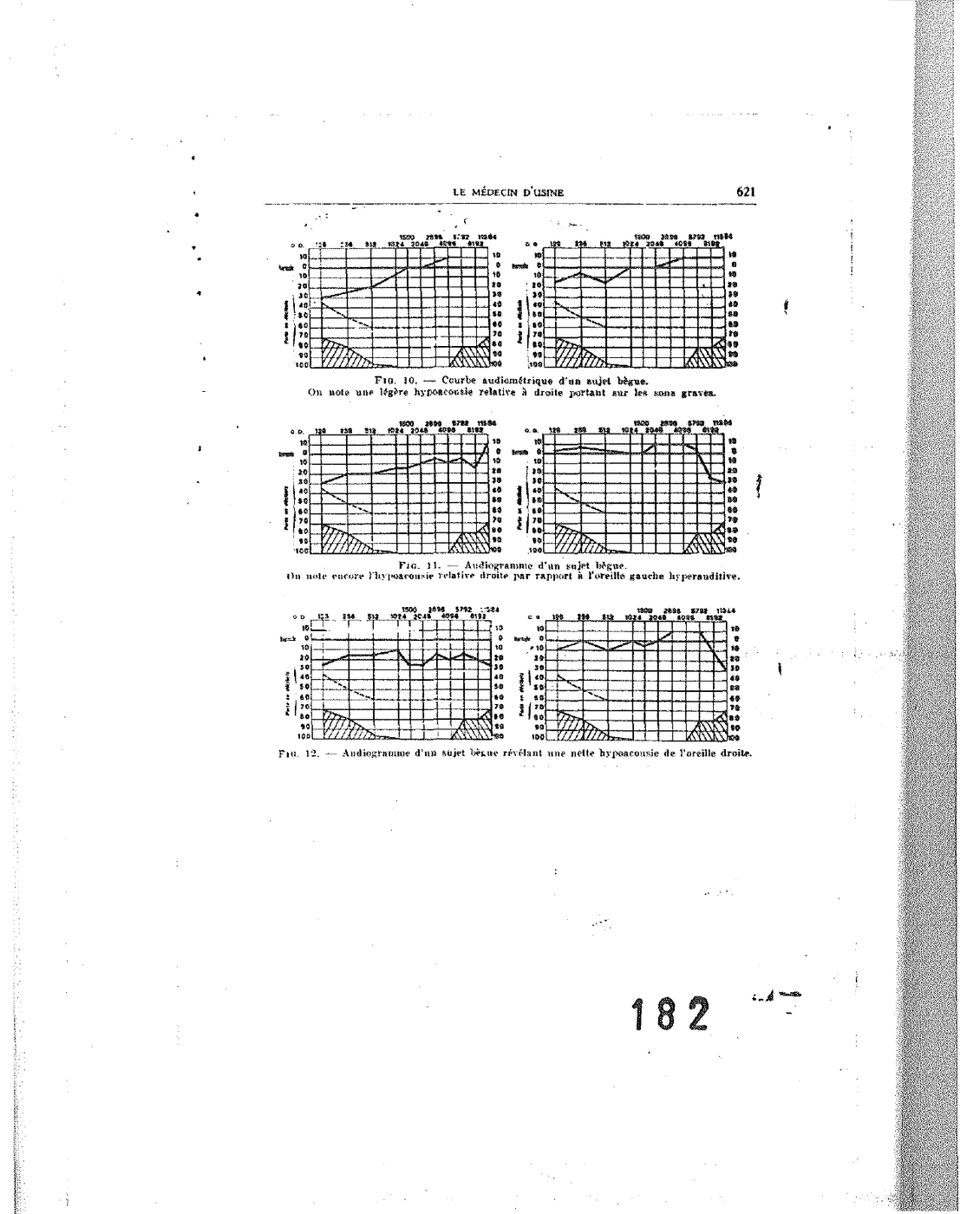
The audiometric examination carefully conducted, when it bears separately on the right ear and the left ear, brings out a constant fact: in the right-hander, the right ear presents a relative hyperacusis with respect to the left ear, particularly clear on the low frequencies. Inversely, the left ear presents, in the left-hander, the corresponding hyperacusis.
This ear — the one that hears the low frequencies better — is what we shall call the directing ear. It commands the rhythm of phonation. Any lesion which affects it durably disturbs the rhythm of the voice, whether it is a question of the spoken voice (delivery, accentuation, articulation) or of the sung voice (accuracy, attack, support). Inversely, any disturbance of vocal rhythm corresponds to an impairment of the directing ear and must be sought on that side.
[Figs. 10 to 12 — Audiograms of right-handed subjects: relative hyperacusis of the right ear on low sounds.]
Stammering constitutes the limit-case of this dysrhythmia. If one artificially lengthens the delay of return of the emitted sound to the ear — by an electronic device introducing a delay of the order of a fifteenth of a second —, one makes a stammerer, in a few minutes, of the most normal subject. Inversely, the careful audiometric examination of stammerers reveals, in the near totality of cases, a characterised auditory dysrhythmia: either a marked asymmetry between the right and the left ear, or an absence of directing ear. Auditory re-education aims to restore the correct dominance.
[Fig. 13 — Audition-phonation circuit in the right-handed subject: right ear → left auditory centre → phonatory organs.]
[Fig. 14 — Audition-phonation circuit in the right-handed subject who has lost his directing ear: transcerebral transfer.]
II. — Timbre disorders
a) Deafness of singers. The audiometric examination of singers — and more generally of professional voice users — reveals, after a few years of exercise, an elective impairment bearing on the high frequencies (3,000-4,000 c/s). This impairment first affects the right ear (the directing ear in the right-hander), then extends to the left ear. It entails a corresponding modification of the timbre, the singer progressively losing the mastery of the upper harmonics which ensure the clarity of the emission.
[Figs. 15 to 17 — Audiometric responses of two singers, and their evolution in time: progressive fall on the right side (directing ear) and then bilateralisation.]
b) Scotomata. One sometimes observes, on the audiogram, very elective falls bearing on a frequency or a narrow group of frequencies, the rest of the tracing remaining normal. These falls — which we call auditory scotomata, by analogy with the scotomata of the visual field — always correspond, in the spectral analysis of the subject’s voice, to vocal scotomata: the voice does not contain either the frequencies that the ear does not hear. This correspondence, constant, furnishes the daily proof of the fact that the voice of a subject contains only the harmonics which his ear is liable to hear.
III. — Auditory selectivity: the racial auditions
The comparative examination of a great number of subjects of different nationalities clearly reveals systematic differences of auditory selectivity. These differences are not anatomical: they are functional, that is, acquired in the course of the auditory conditioning imposed upon the child by the sonic bath of his mother tongue. We propose, to designate them, the term racial auditions.
The Italian ear presents a narrow pass band, centred on the 2,000-4,000 cycles per second zone. It is this acute selectivity which gives the Italian vocal timbre its characteristic clarity and brilliance.
The French ear presents a pass band centred on the 1,000-2,000 cycles per second zone, therefore appreciably lower than the Italian ear. The French vocal timbre finds therein its median colouring, its absence of high brilliance.
The Russian ear presents no elective zone of selectivity: its response curve spreads uniformly from the low to the high frequencies, which accounts both for the harmonic richness of the Russian voice and for the ease with which Russians accede to the most diverse foreign languages.
[Fig. 18 — Selectivity of an Italian ear: the pass band is inscribed between 2,000 and 4,000 c/s.]
[Fig. 20 — Selectivity band of a typical French ear, limited between 1,000 and 2,000 c/s.]
[Fig. 21 — Selective field of a Russian ear, extending from the low to the extremely high sounds.]
These racial auditions are not immutable. They may be modified by an appropriate conditioning, and it is precisely on this conditioning that our method of integration of foreign languages rests — the first results of which are currently in application at the Audio-Visual Centre of the École Normale Supérieure de Saint-Cloud.
IV. — Conclusion
Auditory disorders of occupational origin, long considered as ineluctable fatalities linked to industrialisation, can be both prevented, detected at an early stage, and — within certain limits — re-educated. Prevention falls to the arrangement of premises and to individual equipment; detection falls to a systematic and well-conducted plant audiometry; re-education falls to an objective audiometry, whose foundations have been laid by our work of the last ten years and which we have progressively extended to affections of the voice, to rhythm disorders, and to the integration of foreign languages.
The plant physician occupies, in this device, a key position: it is on him that depends, for hundreds of thousands of workers, the maintenance of auditory integrity — a fragile capital on which rest, more than is commonly believed, psychic balance, sociability, and indeed the very quality of life.
SUMMARY
Occupational deafness develops in four periods — installation of the permanent deficit, total latency, sub-total latency, manifest deafness — of which only the first three are accessible to a preventive therapy. Systematic plant audiometry allows its detection. An objective audiometry, founded on the exploitation of audio-phonatory counter-reactions ("Tomatis effect"), allows the confirmation of the diagnosis independently of the subject’s cooperation, and the exploration of its prolongations: directing ear and rhythm disorders, auditory and vocal scotomata, racial selectivities (Italian, French, Russian), deafness of singers, integration of foreign languages.
SUMMARY
Industrial deafness develops through four successive stages — installation of permanent deficit, total latency, subtotal latency, manifest deafness — only the first three of which are amenable to preventive treatment. Systematic plant audiometry ensures early detection. An objective audiometry, based on the audio-phonatory feedback loop (« Tomatis effect »), provides diagnostic confirmation independent of the subject’s cooperation, and opens up the related fields of directional ear and rhythm disorders, auditory and vocal scotomata, racial selectivities (Italian, French, Russian), singers’ deafness, and foreign language integration.
A. TOMATIS
[Fig. 22 — Whole of the mounting allowing objective audiometry. M: microphone — An: Analyser — Am: Amplifier — E: Earphone. Low-pass, band-pass, high-pass filters. Audiometer.]
Source: Tomatis A., “Les nuisances du bruit — Surdité professionnelle, audiométrie d’usine, audiométrie objective”, LE MÉDECIN D’USINE, November 1957, pp. 605-624. Offprint preserved in Alfred Tomatis’s personal archives. Twenty-two original figures (audiograms, diagrams of the audition-phonation circuit and of transcerebral transfer, electronic mounting of objective audiometry).
Illustrated pages from the original document
Pages of the PDF facsimile containing figures, diagrams or audiograms. Depending on the original layout, certain pages may appear in landscape orientation.
Page 12 of the facsimile
Page 13 of the facsimile
Page 16 of the facsimile