Phonic Preparation for Childbirth
Phonic preparation for childbirth at Foch in 1991
SCHOOL OF MIDWIVES OF THE FOCH MEDICAL-SURGICAL CENTRE
40, rue Worth 92151 SURESNES
End-of-studies dissertation presented by: Caroline D’ORTHO and Brigitte MONNET in view of obtaining the state diploma of midwife, academic year 1991-1992
Acknowledgements
We thank principally Doctor PINET, our dissertation supervisor, as well as Madame TORDJMAN, midwife, who are responsible for the phonic preparation at the Foch CMC.
We wish to thank most particularly Madame SALIN, psychologist and assistant at the Alfred Tomatis centre, for her availability and her listening.
We thank finally Madame NEVEU for her kind collaboration as well as all the patients who responded with kindness to the questionnaires and interviews.
We cannot cite all the persons who have supported us by their help or their interest in this subject, but we wish to name: Sidonie Deltour, Henry Angleys… Thanks to the persons of the Tomatis centre and to the journalists.
Plan
Introduction
First part: Theory
-
Who is Tomatis? His path, his work, his philosophy
-
The Electronic Ear, music and the filtered maternal voice
-
The method of preparation for birth
Second Part: Comparative study
With three groups:
-
A. Tomatis preparation
-
Classical preparation
-
Without preparation
A. Generalities
-
Presentation of the means of work
-
Presentation of the three groups
B. Preparation for birth and pregnancy
-
Anxiety scale
-
Observation based on testimonies
C. Childbirth
-
Comparison of the 3 groups in function of the different obstetric parameters
-
Testimonies gathered postpartum
D. Conclusion
-
Are there significant differences between these 3 groups?
-
Does the Alfred Tomatis method bring a plus?
-
Does it respond to the expectations of women?
Third part: Discussion
A. Is the Alfred Tomatis method satisfying?
-
For the patients
-
For Doctor Alfred Tomatis
-
For the medical team
B. Bias and criticisms
C. Proposals
Conclusion
ANNEXES
-
Hamilton scale
-
Diagram of the Electronic Ear
-
Diagrams of the comparative study
Two developments relating to the Tomatis method: Foetal audition with sonic birth
- The learning of languages by the Tomatis method
Introduction
Obstetricians and midwives, at the service of pregnant women, seek to reunite all the conditions necessary for a harmonious birth. To prevent obstetric and neonatal pathologies is the principal objective of their works. During pregnancy and birth, the psychological and physical aspects are constantly considered. Preparations for birth are proposed to future parents within the framework of this prevention. Numerous, different, complementary… Patients may choose their preparation in function of their expectations, their availability, their personality and the internal organisation of the establishment where they are followed.
Since 1 January 1991, the Foch CMC has proposed to pregnant women a new preparation for birth: the method of phonic preparation according to the Tomatis effect. Set up at the Vesoul hospital since 1988, it remains little known to the general public, to women themselves and to the medical profession.
In order to discover it, it is important to understand its functioning, its principle based on the “Electronic Ear” and its origin. Such is the objective of our first part.
The Alfred Tomatis effect proposed to pregnant women as a preparation for birth must still prove its effectiveness and its interest. It is therefore necessary to seek to define, rigorously, its impact on pregnancy, on childbirth and on the child at birth thanks to a comparative and retrospective study.
Finally, a personal viewpoint will complete this work.
Thus we draw up the assessment of the year 1991 of this new phonic preparation proposed at the Foch CMC.
Part 1: “Theory” — Who is Alfred Tomatis?
A specialist in otorhinolaryngology of the Faculty of Medicine of Paris, Doctor Alfred Tomatis is above all a man. Thanks to his qualities as a researcher, he exercises his functions as therapist by having created a new discipline: audio-psycho-phonology.
Let us make the acquaintance of Alfred Tomatis. Let us discover his research work. Thus we shall better understand his therapy designated by Alfred Tomatis Method or “Audio-psycho-phonology”.
1 — A Man
Greatly premature, Alfred Tomatis was born in Nice on 1 January 1920. In his work L’Oreille et la vie, Alfred Tomatis writes an autobiography. He insists on his prematurity, for this detail would seem to have had significant consequences on his life and his works. “I retain the conviction that the conditions in which I was born contributed to orienting, to a large measure, the works I have pursued until now in the domain of intra-uterine life…” “My vocation as a researcher, I find it in my quality as a premature in quest of a nirvana from which I was excluded far too early.” “A premature child, I am typically the one who, to live, had to set into play at that moment a whole dynamic of exit; the one who, from the outset, had to inscribe his desire to live in an effort. Since then, the very fact of existing is for me indissolubly linked to a generous and quasi-permanent investment of energy.”
He decided to be a doctor very young, from the age of 9.
“I too will be a doctor. I too will be a man who searches for what he does not know.”
He associates medicine and research “in quest of humanisation”.
Encouraged by his father and conscious of his vocation, he sticks to his work. He calls himself “a fierce, indefatigable plodder”.
He adds to his scientific formation a medical specialisation: otorhinolaryngology. Tomatis himself explains his choice to us: “I had very early been made aware of certain difficulties encountered by singers, friends of my father, and I would have liked to find solutions to their problems, which the medicine of the time seemed in little hurry to settle. It was doubtless ambitious, but it was also a good way of investing the filial affection that had always supported me — not to say inspired me — during my studies at the lycée and my university work.”
To understand his path, it is necessary to evoke his father. He speaks of him with admiration and gratitude.
“I have always perceived my father as an exceptional being.”
“All that I owe him, I cannot even evaluate.”
“My father was a precious ally… And more than that even, he was an ear: someone who was always ready to hear me and who, more than anyone else in my entourage, truly listened to me.” His father was a theatre man, a singer and a lover of music.
Tomatis grew up in this world and acquired an incontestable knowledge of it.
“When my father came to Paris, I was saturated with music — saturated but happy.”
“Frequenting my father… led me to share this life behind the scenes of the theatre, so rich in teachings of all orders. In the wake of a great artist, I was not only assimilating the repertoire, I was also integrating the psychology of the singers of the time and of their public.”
A man of will, a worker thirsting for knowledge, lulled from the earliest age by theatre and singing, Alfred Tomatis says of himself that he is emotional and observant: “It is from the perception and analysis of what happens around me that I draw my greatest joys. This disposition has rendered me enormous services, both in research and in the clinic.”
2 — A Researcher
An otorhinolaryngologist and consulting physician at the Aeronautical Arsenals, he was able to observe a great number of persons submitted to noise. He speaks of acoustic aggression.
He carries out his first investigations, accumulates observations and measurements based on audiometric tests. Later, these various parameters seem to him subjective. The psychological conditions of the persons submitted to these tests would modify the results. Tomatis therefore invents a listening test.
“… A listening test on which psychological dimensions, somatic data and behavioural reactions with the environment were inscribed.”
He seeks to make audiometry more objective.
Audiometry studies the auditory thresholds of the individual. The listening test seeks in addition the auditory laterality and the selectivity of the ear. Its analysis allows the definition of the subject’s dominant ear and the knowledge of his capacity to differentiate sounds between them and in space. The listening test is therefore an interpretation of the subject’s listening and bodily schema, while audiometry analyses only the capacity of a subject to hear. The listening test is the basis of Tomatis’s works.
Thanks to and for his father, he seeks to come to the aid of singers who have damaged or lost their voice. In studying the auditory curves of these singers, he observes that they presented deficiencies observed in subjects afflicted with occupational deafness. He deduces from this that “singers ‘broke their own ear’”. They remained deaf. As his works progress, asking himself why patients sang out of tune, he ends up advancing:
“A subject reproduces vocally only what he is capable of hearing.” The ear then appears to him as the fundamental instrument of phonation. We are in 1947.
Thus, to improve his voice, one must correct and/or perfect listening. His works orient themselves in this direction, and he defines the physiological parameters constituting listening:
-
The bony transmission of sounds
-
the time of setting to listening of the body
-
the time of setting to listening of the ear — that is, the gating system
-
the auditory lateralisation with the directing right ear.
These laws govern audio-phonatory self-monitoring. They are patented under the name “Tomatis effects”. They are at the basis of the Electronic Ear.
- The Electronic Ear is an apparatus conceived by Alfred Tomatis allowing him to impose upon a subject a certain auditory curve — that of a perfect ear. Thanks to this technique, he re-educates listening — which, disturbed, entails numerous disorders.
We shall return to these various notions later, for they are important to understand in order to define the Alfred Tomatis method.
- If the voice is defined as an emission of sounds, it is above all a means of communication thanks to language. Naturally Alfred Tomatis wonders about the origin of language and the desire to communicate.
He answers thus:
“It is born above all from the desire not to rupture (or eventually to renew) the sonic relation maintained with the mother during prenatal life.”
We see then how Doctor Alfred Tomatis was led to explore prenatal life. His works on foetal listening begin around 1962.
We shall refer to the annexes for more details on this subject, but we shall retain here three elements:
-
The foetus hears and memorises sounds. The ear is functional from 4 and a half months of pregnancy. It is the first sensitive organ which will accumulate all the history and affective imprint of the pregnancy.
-
During pregnancy there unfolds for the foetus a primordial experience of perceptions and sensations. The mother’s voice has a privileged role. It is the basis of all the later affective and emotional organisation.
-
The auditory function evolves; maturation due essentially to the passage from a liquid milieu to an aerial milieu. The dynamic at the origin of this adaptation of the ear is guided by the search for the maternal voice. It is the continuation of the communication established in utero.
Alfred Tomatis confirms that the maternal voice has an impact on the evolution of a child’s desire to communicate through what he calls sonic birth. It is a therapeutic method whose aim is to allow the individual to recover the desire to communicate and therefore to correct his relational disorders.
Through this chapter, we have evoked notions on which Tomatis still today relies to propose help, support or therapy:
-
listening test: language is closely linked to listening
-
the Electronic Ear
-
desire to communicate: the desire to live takes its source in the intra-uterine universe
-
the mother’s voice guides the child towards communication:
-
the psychic and sensory life of the foetus is an invitation for his future life
These points allow the comprehension of the Tomatis method. They come from works, observations and tests. Thanks to this research, Tomatis is also a therapist.
3 — A Therapist
Alfred Tomatis’s works have only one aim:
-
To come to the aid
-
to allow a better humanisation, to take up his terms.
Such is the origin of his vocation as researcher.
His therapeutic schemes address children, adults but also pregnant women. The indications are variable and multiple. But all are based on the quality of listening and therefore on the Electronic Ear, for if the indications are diverse, all find their origin in listening.
We shall therefore refer to the paragraph “Fields of application of the Electronic Ear” to discover Tomatis the therapist.
The Electronic Ear
Definition: Generalities
The voice and listening, according to Alfred Tomatis, represent two functions dependent on one another. One would be controlled by the other and vice versa. We have just redefined the elementary notion on which the Tomatis effect rests: self-monitoring. Now one must self-monitor in order to hear like a great professional of the voice. From this necessity was born the Electronic Ear:
-
a machine permitting this learning
-
an apparatus seeking to reproduce exactly the way of hearing of a very good ear
-
a process permitting the acquisition of a listening posture.
It is therefore a “machine”. It has benefited from the progress of technology. Today it is composed of:
-
an electronic gating
-
amplifiers
-
a double-output headset with vibrator and earphones corresponding to the dual bone and air conduction
-
microphones (refer to the diagram of the Electronic Ear in the annexes)
Without developing in more detail the technical aspect of the Electronic Ear, we must retain that this arrangement allows a re-education of the ear by obliging it to hear a sound in a certain way upon the emission of a sound. This auditory conditioning is achieved by exerting a tension of the tympanum obtained thanks to the regulation of the two muscles of the malleus and stapes, by imposing upon the subject a certain band of frequencies with a lateralisation on the directing right ear.
We have just defined in a general way the Electronic Ear. Its functioning is based on fundamental principles to which it seems interesting to return. Thus, we shall understand what “hearing well” is for Tomatis. We shall therefore envisage:
-
The directing right ear
-
the gating system
-
the filtered sounds
-
and finally: “Why Mozart?”
Basic Principle
a) The preponderant role of the right ear
This importance finds its source in physiology. The innervation of the right ear conducts acoustic perception to the level of the left auditory centre. Now the centre of verbalisation — in other words, the motor centre of the larynx — as well as the zone of language comprehension is situated in the left hemisphere. The audio-phonatory circuit is therefore a direct circuit.
A notable asymmetry is noted at the level of the innervation of the larynx. The self-listening system is therefore shorter on the right. These two anatomical elements explain that, by its innervation, the right ear is much closer to information than the left ear. It is therefore more invested in language. One may say that the right ear aims at a precise sound, is more sensitive to high frequencies. The left ear gives an overall panorama of the sonic environment and captures the low frequencies better.
Beyond this anatomical dimension, we recall a psychological notion: the dynamic of the right over the left. They have a different symbolic value. The right represents monitoring, supervision and the future; the left, affect and the past. It is appeasing that emotions be monitored for a better equilibrium. Alfred Tomatis observes that a pregnant woman with a left dominant ear — diagnosed thanks to the listening test — is very anxious. So he proposes an auditory support by the Electronic Ear in order to lateralise her right ear: her right ear will then be dominant.
Dyslexics, left-handed of the ear, correct their disorders after having submitted to sessions under the Electronic Ear. Thanks to this re-education of listening, the right ear will be dominant.
These two examples illustrate the following self-evidence: communication is easier if anxieties are minimised and if phonation is clear.
To be well lateralised — which means to have a dominant right ear — conditions good listening.
b) The gating system
To understand the functioning of the Electronic Ear, let us recall the two types of sound conduction:
-
Bone conduction: through the intermediary of the cranial vault, the vibrations inform the auditory nerve.
-
Air conduction: direct conduction. The vibrations of the tympanum reach the inner ear which informs the auditory nerve.
There exists a time of latency between the two types of transmission. The sound arrives directly at the inner ear by air conduction. To capture this sound, “the ear must in a way be ready to listen”. This is achieved by the bony pathway. It is the time of setting to listening of the body.
Good listening will only be obtained through the intermediary of a dynamic statics, a verticality of the person, as well as a dynamic of the middle and inner ear: a tension of the two muscles of the malleus and stapes in order to prepare the tympanum to gather the sound. The Electronic Ear allows the ear to hear in a better way thanks to its gating system between bone and air conduction. This leads to diminishing the time of latency.
-
Bone conduction is favoured by a vertical statics of the person
-
air conduction is facilitated by the quality of the auditory canal composing the outer ear and by the tension of the tympanum.
Now the listening of filtered sounds, rich in high frequencies, contributes to the more effective work of the muscles of the middle ear. It is a re-education of the tympanum.
To listen well is also to reduce to a minimum the time of latency existing between bone and air conduction of a sound.
c) Filtered sounds: sonic universe of intra-uterine life
Besides the lateralisation of the right ear and the gating system, the listening of filtered sounds is indispensable to the conditioning of the Electronic Ear.
-
They play directly on the muscular tension of the tympanum: the higher the sound, the more the tympanum is tense. The filtered sounds activate the muscular system.
-
Emission of sounds in an aquatic milieu,
-
scotomisation of low frequencies in the laboratory.
We know that the foetus hears. It memorises sounds. The foetal ear is operational from four and a half months of pregnancy. It bathes in a universe of sounds where the maternal voice has primordial importance: beyond the semantic, it communicates the affective.
Thus, filtered sounds permit:
-
A reminiscence of the uterine milieu in its securing aspect — well-being, harmonious blossoming.
-
A very dynamising aspect engendered by the high frequencies.
Auditory stimulations by high frequencies improve cerebral tonus, give an opening of consciousness, solicit all the participation of the subject. Alfred Tomatis designates this effect by the term: verticality.
Through the ear, the filtered sounds touch the individual in his globality. An equilibrium is achieved between an appeasement and a solicitation of all the energy of the body and consciousness.
d) The choice of sounds
Alfred Tomatis filters sounds from the maternal voice and the works of Mozart. Let us study this selection.
The Electronic Ear sends filtered sounds to a subject in order to effect a pedagogy of listening. This is achieved by an auditory conditioning that seeks to send back to intra-uterine listening. This intra-uterine sonic environment is essentially invaded by the maternal voice. We therefore understand why Tomatis records and then filters the maternal voice. Heard again under the Electronic Ear, it restitutes the affective charge indispensable to arousing, accelerating or restoring in a child the desire to communicate — the desire to live. The maternal voice is used for a therapeutic purpose. Tomatis insists much on the maternal voice. It is at the origin of a foetus’s desire to live, through the love it transmits.
The maternal voice is not always usable or desirable. Alfred Tomatis then uses musical sounds. According to his clinical experiences and his laboratory trials, the works of Mozart — above all the pieces for violin — have Tomatis’s preference. They allow the obtaining of the same effects as the maternal voice. The results are astonishing, always positive, in all corners of the world and whatever the ethnic group concerned. “Mozart’s music is universal”, declares Alfred Tomatis. He adds: “Mozart is a genius composer.” Let us not forget that Tomatis knows music.
He has worked with other composers but the results were not as conclusive. Mozart, retransmitted in filtered sounds and listened to under the Electronic Ear, becomes a vector of harmonisation, dynamisation, awakening and creativity. The responses are immediate: the subject becomes active, modifies his neurovegetative references, sees his respiration amplify, his pulse accelerate… He manifests a desire to communicate with his environment. Mozart’s pieces for violin contain numerous sequences rich in high sounds. Now the sonic universe of a foetus is essentially composed of high sounds above 8,000 Hertz. Mozart is used for a therapeutic purpose but also in a work of support.
A third sonic element, but unfiltered, is used in alternation: the Gregorian chants. The modulations here too possess an incontestable universality and pedagogical and therapeutic effectiveness. Contrary to Mozart’s music, Gregorian appeases, calms but also solicits verticality.
Alfred Tomatis uses in certain cases the nursery rhymes of the ethnic group to which the child belongs. They seek to induce a linguistic dynamic when children manifest language disorders. The rhythms they contain prepare to accept language with its psycho-affective incidences liable to transform its relational environment.
The filtered sounds project the subject submitted to the Electronic Ear into the intra-uterine universe. These sounds act on the genesis of the desire to communicate and therefore to live. For Alfred Tomatis, language disorders are among other things the consequences of the disorder of the desire to communicate.
The Electronic Ear, technically, is capable of adapting an auditory conditioning according to the therapy to be carried out — an approach proper to each person. This conditioning is modulated according to the auditory lateralisation and the time of latency defined by the gating system. The choice then falls to the therapist to send filtered sounds obtained from the maternal voice or the works of Mozart in alternation with Gregorian chants and/or children’s nursery rhymes. The therapist must establish a pedagogical scheme based on the disorders observed in the individual and the results of the listening tests to which he has been submitted.
Let us see what are the fields of application of the Alfred Tomatis method. Already let us signal that this method proposes a work of therapy but also a work of support. It must then be envisaged and approached as an aid. It is in this framework that the preparation for birth is situated. We are not faced with a pathology. We shall return to this aspect later.
3 — Fields of application
-
Alfred Tomatis proposes to re-educate the voice of great opera singers by teaching them again to listen with accuracy — that is, to restore to the right ear all its possibility of self-monitoring.
-
Through his consultations, he has been able to analyse numerous auditory curves, thus observing that the various human groups each have a quite particular way of using their ear. Each being sensitive to a certain frequency band — that is, of selectivity. This is explained by the different impedances, air resistances to sounds. Rich with this observation, the Electronic Ear will allow the facilitation of the learning of foreign languages by opening the ear to a certain frequency band characterising a language:
-
French: 1,000 to 2,000 Hertz
-
Italian: 2,000 to 4,000 Hertz
Thus a Frenchman will be able to learn Italian quickly by listening to it like his mother tongue. We develop this application in more detail in the annex.
-
Alfred Tomatis is led to treat children in whom he notes a large number of difficulties in reading or writing. He sees writing as the first magnetic tape and elaborates, thanks to the Electronic Ear, a treatment for dyslexia for example. Beyond these school difficulties, Alfred Tomatis proposes support with an individualised programme to these children in relational difficulty such as the autistic, the characteriological, the stammerer, etc. For Alfred Tomatis, it is a therapy in view of his clinical results. Schematically, the origin of these disorders is a distortion of communication. He proposes, thanks to the Electronic Ear, to relive the passage from liquid audition to aerial audition. This is what he calls sonic birth. It is a treatment elaborated from the listening of sounds increasingly filtered until obtaining frequencies above 8,000 Hertz equivalent to intra-uterine listening.
-
Alfred Tomatis works essentially with children but also — for the children — with the parents. Let us not forget that the maternal voice is primordial in the child’s desire to communicate. On the cover of one of his numerous works, L’Oreille et la Vie, we can read: “He calms the anguished, calms the nervous, balances the unstable, fights against overwork, stammering, ringing of the ears and spelling mistakes. He makes one sing in tune, teaches one to read well, raises failing wills and restores memory to those who have lost it.”
But finally he does only one thing: he teaches one to listen.
From this, the fields of application are immense. Language learning is a good example. Preparation for birth is another, for to listen well is perhaps a necessary element for:
-
Living one’s pregnancy well
-
communicating well with one’s baby
-
giving birth well
-
welcoming one’s baby well…
The two applications do not represent a pathological situation. It is a question of support. From this point, we may ask:
-
How have we come to think of a preparation for birth according to the Alfred Tomatis method?
-
What may be the repercussions of a pregnancy lived “under” the Electronic Ear?
-
How is it put into practice?
Preparation for birth
1 — Origin of the phonic preparation
Although he is the author of La Nuit utérine, a work describing the intra-uterine environment of the foetus, Tomatis is not directly at the origin of the phonic preparation. The elaboration, from intra-uterine life, of communication is a theory brought to light from his works. It is the basis of his therapeutic principle under the Electronic Ear. But this method applied to pregnancy — we owe it to a midwife and an obstetrician.
Having been seduced by the theory and desirous to improve the courses of preparation for childbirth, the service of Professor KLOPFENSTEIN, in a maternity hospital in the east of France, attempted a preparation under the Electronic Ear. We were in 1987. This initiative was received with much reservation and scepticism by the nursing staff.
The midwife, Marie OUVRARD, had had a presentiment, during her years spent in Morocco, of the importance of singing and dancing in this culture as well as the impact this could have at the moment of birth. Indeed, she observed numerous quite harmonious births while no structure of preparation courses existed there. The preparation emanated in a way from their cultural tradition, assuring a physical and psychological well-being to the pregnant woman. From this important place of music for body and mind, interest was aroused for a phonic preparation in France.
To assure women relaxation and dynamism so that they feel at their best during their pregnancy. To live well the beginning of communication with the child and from there to bear an influence on the moment of birth.
Alfred Tomatis, for his part, sees in this preparation a way of improving the development of the child through a harmonious, enriched and stimulating communication thanks to the maternal voice. As audio-psycho-phoniatrician, he wishes to carry out a longitudinal study, therefore over a longer term, relating the behaviour of the child up to his opening to the social through language and schooling.
The basic technique of the Electronic Ear is in no way an experimentation. Pregnancy is a new application of it. It is a finished product that he delivers to us, a material placed at the disposal of the public, that one must use well. It is up to midwives to develop it. The Tomatis centres are pilot centres which do not wish to develop this preparation themselves. But they allow women who wish it supplementary sessions. They propose to obstetricians and midwives to train themselves for the analysis of auditory curves, the adjustments of the Electronic Ear… Projects: Vesoul, Foch, Les Diaconnesses…
2 — Aims
Based on the work of the Electronic Ear, the listening sessions must allow the woman to relax and to recover a better dynamic. Pregnancy invested with such energy and such balance would allow the establishment of a harmonious communication with the foetus. From this communication would spring the desire to know the world, the foetus’s desire to live!
They in no way replace the courses of information and respiration relating to childbirth taught in the so-called classical preparations. The Electronic Ear is an apparatus placed at the disposal of the public, a complementary means of preparing for the birth of one’s child.
The principal objective is to minimise anxiety in order to favour the mother-child relation, without however denying the structuring role of this anxiety necessary to accept childbirth, the bringing into the world, the separation from the imaginary child…
It is natural to wonder about the aims of this method of preparation, but let us distinguish two aspects:
- what we expect from it:
According to the theory and therapeutic experience of Alfred Tomatis himself, we may hope from it such or such effects:
- what we observe:
According to experience, observation and analysis of objective elements, we may conclude that the phonic preparation indeed has such effects on pregnancy, on labour, on expulsion…
We shall try to define what we may expect from the phonic preparation in a first stage. The second part of this work will dwell on the second aspect. Then we shall try to put them in parallel in order to conclude.
If we may think that the phonic preparation minimises the anxieties of pregnant women, we may hope for a better well-being of childbirth:
-
Diminution of the time of labour,
-
Diminution of the number of caesareans,
-
Diminution of the rate of instrumental interventions,
-
Diminution of chronic and/or acute foetal sufferings — the experience of the Vesoul maternity seems to orient itself in this direction.
Beyond childbirth, can we hope for a better well-being of the child? Such are Alfred Tomatis’s expectations. Indeed, pregnancy lived under the Electronic Ear facilitates mother/foetus communication, therefore favours the desire to communicate of this foetus becoming child, adolescent… Whence a better awakening, a good psycho-motor development, a better socialisation. We imagine the difficulties to be overcome to establish a longitudinal study allowing the obtaining of objective results — but, with more hindsight, shall we one day be able to answer this question?
3 — Means
The basic principles of the Electronic Ear remain the same. By a gating system, it will achieve a double work on the ear to optimise active listening. The apparatus, as the sessions progress, ensures:
-
A better verticality: the body is set to listening.
-
A diminution of the time of latency so as to open the ear to sounds.
The filtered sounds (high and middle) will contribute to making the muscles of the malleus and stapes work to tense the tympanum… Through an auditory lateralisation to the right, one allows the improvement of statics (control of balance) as well as a mastery of language.
-
Gating air-bone conduction.
-
Lateralisation — right ear.
-
Filtering.
Three pillars of the Alfred Tomatis method to improve the mother’s voice.
4 — Importance of the maternal voice in the sonic environment of the foetus
We have already had occasion to evoke the maternal voice. We allow ourselves to return to it in order to bring some information. They again come from Alfred Tomatis’s works.
The foetus lives in a sonic world since it is surrounded by the respiratory, digestive, cardiac movements of its mother. But happily, low-frequency sounds have a very poor bone conduction. Moreover, air conduction is very muffled. To traverse the abdominal wall, approximately 110 decibels would be needed — the equivalent of a loudspeaker. The foetus therefore perceives sounds principally by bone conduction. The harmonics of high frequencies are perceived in a privileged way. There is even an amplification of the high and middle frequencies through this transmission pathway.
“When the larynx vibrates, the spinal column reacts like the string of a bow. The pelvis becomes an enormous resonance chamber.”
The foetus is lulled during the pregnancy by the voice of his mother, amplified. It does not reach him distinctly. It is the modulations, the harmonics, the timbre of this voice that the child seeks to recover at birth. He also perceives all that the mother hears, transmitted by bone conduction. Thus, the mother is an ear which opens the child to the universe.
5 — The place of the father
For Alfred Tomatis, the father’s voice is perceived by the child on the same basis as all surrounding sounds by bone conduction but in an attenuated way relative to the maternal voice which vibrates directly upon his body. But if the mother receives the father’s voice in a positive way, in attentive listening, she will transmit it to the foetus. He will receive it differently if this same mother is reticent towards the father. The role of the father is also to support his wife in her role of mother. For Tomatis, the place of the father with respect to the foetus and the young child intervenes indirectly through the blossoming of the mother; it thus has all its importance.
6 — In practice
The application of the phonic method at Foch is set up since January 1991 thanks to the Electronic Ear with the participation of Mr PINET and Madame TORDJMAN. It has been established according to the following criteria: two listening sessions per week for five weeks; around the eighth month of pregnancy, sessions of filtered sounds from Mozart alternating with Gregorian chants. This phonic preparation is proposed to interested women, in complement to the classical courses.
The headset:
Reproduction of the way of hearing of a very good ear.
Lateralisation:
-
Allowing work on equilibrium, the setting to listening of the body in dynamic position
-
allowing better self-monitoring of the maternal voice.
This right-side lateralisation is important in the pregnant woman. We recall that the right cerebral hemisphere is linked mostly to the left ear. It represents the brain of emotions and the affective. With a dominant left ear, the pregnant woman risks being submitted to too great anxieties. So one must re-balance, reinforce the work of the right ear and the left brain. Moreover, this right-side lateralisation accentuates motor and psychological dynamism.
The gating system:
By diminishing the time between air and bone conduction. There is progression over the course of these sessions: the time of latency is shorter and shorter.
The filtered sounds:
Scotomisation of low frequencies and passage into a liquid milieu. They ensure a well-being, an appeasement, a reminiscence of intra-uterine security. The high sounds stimulate the cortex and ensure a tympanic tension through muscular work.
The sessions of phonic preparation follow a common, pre-established programme. This method being at the origin a therapy, the listening of filtered sounds in an excessive or non-adapted way would risk reawakening affects in certain women. Such is not the aim of this phonic preparation. Beforehand the pregnant women therefore submit to an audiogram. This test excludes auditory pathologies. The maternal voice is never used. In contrast, the music of Mozart is filtered. It is so progressively and weakly relative to a programme determined for a therapeutic aim. It is played in alternation with unfiltered Gregorian chants. The rhythms facilitate appeasement and calm.
The periodicity of this preparation is an important factor. One may be astonished at the rather short lapse of time over which the sessions unfold. Through this programme, a work on the right ear is effected. Listening and the maternal voice improve. Normally, this phenomenon maintains itself beyond the sessions. The mother recovers, thanks to these sessions, a dynamism and an activity which allow her to be participating. But she must not be dependent on the Electronic Ear. Moreover, too many sessions could produce the inverse effect, entailing a saturation of the ear.
Alone and spontaneously, the mother realises and participates in the continuity of the preparation up to childbirth and beyond. By a better posture, her voice transforms itself, becomes more tonic, more timbred and more modulated. By speaking with her child, she will maintain this work. The Vesoul clinic and the Alfred Tomatis centres propose other rhythms:
-
At the sixth month of pregnancy for fifteen days, 1 hour to 1 hour 30 of session under the Electronic Ear per day.
-
Then at the eighth month for eight days.
It is a more in-depth work. But these two support approaches have the same aims.
Let us evoke the group aspect of this preparation. A phenomenon of emulation is observed. The dynamic of the group and the sharing between women seem facilitated:
-
They evolve at the same rhythm.
-
They find themselves always in the same group and frequently
A certain “conviviality and fraternity” is noted.
“It is another way of coming to the hospital, neither for a consultation nor for an examination”.
“We feel freer”.
“It is easier to speak to the midwife than in consultation”.
But we may wonder if this interest is proper to the phonic preparation. The phonic preparation allows the pregnant woman to refine her listening and therefore would facilitate her communication with others. The dynamic of a group in phonic preparation could be well influenced thereby.
Second Part: Comparative study
Generalities
1 — Presentation of the means of work
The Electronic Ear applied to the pregnant woman in the framework of a preparation for birth seems promising on the theoretical plane. From the analysis of concrete elements, we research the influence of this preparation; a comparative study may therefore be established with rigour and objectivity. For this we use:
the anxiety scale or Hamilton scale: (see annex)
It allows the quantification, by means of a score, of the anxiety of an individual. It has been used for many years by psychologists and psychiatrists. In order to be better adapted to the pregnant woman, the items have been slightly modified. They are five in number. The patient evaluates from 0 to 4 each of them in function of the intensity of the clinical symptom described. This scale considers the repercussion of anxiety.
-
On intellectual functions (difficulty of concentration).
-
On mood (waiting for the worst, irritability),
-
on insomnia (painful dreams, night terrors),
-
on the cardiovascular system (palpitations, sensations of fainting),
-
and on gastrointestinal symptoms (weight on the chest, sensation of suffocation).
The total of these five items therefore ranges from 0 to 20; a note representative of the patient’s anxiety. The patients fill in this scale at the beginning and at the end of the preparation sessions for childbirth. This reflects the evolution of their anxiety under the influence of the preparation.
Two groups are constituted:
-
group of classical preparation
-
group of A. Tomatis preparation
We therefore compare the anxiety scales of these two groups. With the help of these scores, we study the repercussion of the phonic preparation on pregnancy.
The obstetric files
Every patient followed at the maternity of the Foch CMC has her obstetric file. It records her antecedents, the unfolding of her pregnancy and birth as well as the paediatric surveillance of her child. The file is totally computerised. Thus, data are gathered and classified in function of the type of preparation for birth. The global population of primiparas followed at the Foch CMC over the year 1991 is therefore grouped in three sets:
-
a group of 245 unprepared
-
a group of 683 prepared by the classical method
-
a group of 53 prepared by the Alfred Tomatis method
The computer data are compared and treated according to statistical methods. They have allowed us to define the 3 groups, to compare the births and the state of the children at birth.
The visits and testimonies gathered postpartum
Ten women prepared for birth by the Electronic Ear were interviewed postpartum. They confided to us impressions of the phonic preparation. They recounted to us the memories they have of their pregnancy and birth. These testimonies bequeath us data calling upon our subjectivity but many overlap. They have therefore been exploited in order to define the motivations of women and in the more personal part of our work.
2 — Presentation of the three groups
Epidemiological data
Here are some epidemiological data to complete the presentation of our study on the preparation for birth by the Alfred Tomatis method.
The medico-social characteristics such as age, professional activity, medical and gynaeco-obstetric antecedents will allow us to define a profile of the woman of the A. Tomatis group, compared to the global population of the Foch CMC.
The “A. Tomatis group”, as we have named it, represents the pregnant women followed at Foch and having chosen to participate in the course of the eighth month in a complementary phonic preparation. Over the year 1991, the number is 58 parturients, that is, 5.4% of the patients having given birth at Foch that year (cf. annex, Figure 1).
The distribution according to parity
It shows us significant differences in the three groups (see figure 2 in the annexes).
- With a strong proportion of primiparas: 91.4% in the A. Tomatis group against 63.7% in the classical group.
This near-totality of primiparas echoes the motivations of women having chosen this preparation — “to do everything to succeed in my pregnancy” — but many wish to renew the experience for a future pregnancy.
-
Few multiparas therefore chose this preparation: 8% against 36% in the classical group, perhaps related to the time constraint. But it is also noted that few multiparas follow a preparation: 2/3 of multiparas in the group without preparation. So the time factor also intervenes for the classical preparation but in a less marked way, since the phonic preparation is necessarily complementary to the courses of general information and learning of respiration. From this observation, one might perhaps draw conclusions as to the time arrangement fixed. Possibly think of offering more flexibility in the organisation of the phonic sessions.
-
53 women in the A. Tomatis group
-
683 women in the classical group
-
245 women in the group without preparation
The age averages
appreciably different:
-
A. Tomatis preparation: 30 years
-
Classical preparation: 28 years
-
Without preparation: 26 years
It should be noted that this average is surprising given that the distribution according to parity is inverted, since 2/3 of multiparas are in the unprepared group.
The profile of the Tomatis group therefore appears as primiparas with a slightly higher average age.
Professional activity
To exercise or not during pregnancy (refer to figure 3 in the annexes).
Groups 1 and 2 are homogeneous. For the whole of women following courses:
-
85% exercise their professional activity during pregnancy.
-
do not work habitually
-
hospitalised, on strict rest
The percentage of unemployment is minimal: 1.7%. It does not appear in the A. Tomatis group but this has nothing significant about it. This difference of distribution is striking in the group without preparation, since twice as many women exercise no professional activity during pregnancy. These figures are certainly in correlation with parity (2/3 of multiparas in this group).
The distribution according to professions
as a reflection of the socio-economic level of the group
Does the Alfred Tomatis preparation, based on the listening of music of Mozart and Gregorian chants, attract women of a more favoured socio-economic level? Or has this preparation through the information given about it in consultation reached all social milieus in an identical way? What sociocultural profile is more attracted by this kind of preparation? The distribution of the A. Tomatis group according to the professional activity of the patients is schematised by figure 4 in the annexes.
To compare the socio-economic milieus between the different preparation groups, we have chosen the criterion of the level of study. The computer data have thus allowed us to draw up a profile of each group, represented by diagram 5. The figures speak for themselves. We have nonetheless taken care to verify whether they were significant or not.
What does one observe?
-
A very strong majority for the A. Tomatis group: 68.77%
-
an average rate in the classical preparation group: 50.37%
-
a lower rate for the unprepared group.
See Diagram 6.
In the three groups, the percentage of university studies, despite these differences, always represents the highest rate.
- The percentage of the level of technical studies is similar around 18%, whatever the preparation. Nevertheless, it comes in second place by order of importance in the A. Tomatis group. In the two other groups, it is less important than the percentage of secondary studies level.
Remark: This classification seems erroneous to us. Why put the technical aside when it can be studied as much in university (DUT) as in secondary school (BEP)?
-
In the groups of classical preparation and unprepared, the level of secondary studies represents about a quarter of the effectives. In the A. Tomatis group, it represents 1/8. So in a significant way, the percentage of secondary studies of the group without preparation or of classical preparation is the double of the A. Tomatis group.
-
The level of study limited to primary has a very strong percentage in the group without preparation: 12.62% against 2.96% in the classical preparation group. On the other hand, it is the only group where a rate of illiteracy appears: 18.9%.
Antecedents
Concerning medical antecedents, it has not seemed interesting to study them in detail. No particularly striking figure seems to characterise one group more than another. Moreover, the maternity of the Foch CMC does not have a specific recruitment in pathology.
Here are only a few figures from the obstetric antecedents. Thinking that the initial anxiety noted in the A. Tomatis group could be explained by heavier antecedents, we have compared voluntary terminations of pregnancy and miscarriages:
-
The voluntary terminations of pregnancy in the prepared groups are similar, at a rate of 21% on average (number of VTPs related to the number of women). This figure is significantly higher in the unprepared group: 26%.
-
5.2% in the A. Tomatis group
-
19.6% in the classical group
-
27% in the group without preparation
These figures are significant. The hypothesis advanced to explain these differences is the distribution according to parities.
Our initial supposition is therefore not confirmed. The A. Tomatis groups and of classical preparation are similar as to the antecedents. It is neither the number of voluntary terminations of pregnancy nor that of miscarriages which would explain the higher anxiety scored by the Hamilton scale at the beginning of the preparation.
Conclusion
In response to the question that a patient had evoked during an interview: “The atmosphere of the two courses is completely different. Perhaps it is not the same persons?”. The answer is affirmative.
According to the epidemiological data, the profile of the A. Tomatis group appears with:
-
a large majority of primiparas
-
a slightly higher average age (28 years)
-
a higher socio-economic milieu
Motivation for a preparation
To complete the objective description of the A. Tomatis group, we went to meet some patients to better know their motivations relating to the different preparations.
One may say that at base every preparation has as its objective a better experience of pregnancy then of birth… and therefore has a significant impact through the means it has set itself on the elaboration of the mother-child relation.
- What patients seek in a classical preparation:
-
General information on pregnancy, in particular on the epidural, a knowledge of the places, persons, a meeting with the midwife, possibilities of discussion, practical advice (when to come to the hospital?)
-
Exercises on respiration to relax during pregnancy but above all in view of childbirth.
In practice:
The preparation responds to the expectations of women. They are courses condensed in time and in numbers where the personal approach has little place.
- What are the motivations of women who chose the Alfred Tomatis method?
-> In the majority no one knew Doctor Alfred Tomatis. They were informed of this preparation by the information leaflet displayed in consultation, or sometimes by a friend or in the press.
-> A few phrases from the women met postpartum:
-
“I wanted to do a little extra. I felt guilty for not being able to relax (Move). I wanted to do something for my child and to be rested was the simplest thing I had to offer him.”
-
“I had a lot of available time. I was interested in everything that is preparation — relaxation.”
-
“For my first pregnancy, I followed courses of sophrology. There, another preparation was proposed to be well relaxed. I wanted to try.”
Preparation for birth and pregnancy
Introduction
Thanks to the analysis of objective elements, coded in the Hamilton scale, this part is concerned with the contribution of the phonic preparation on the experience of pregnancy. The anxiety scales have been proposed at the beginning and end of preparation to two groups of 50 women:
-
Some having followed the classical preparation at Foch,
-
the others having chosen in complement the A. Tomatis method.
The analysis of these statistical data will allow us to observe the starting groups, their evolution and to note their particular, significant traits. Let us first observe the starting groups. Can we note a particular profile in women who wished to do the phonic preparation? Taking into account the global average score, there exists a significant difference at 3% between these two groups.
The scores reflect the total of the five items rated from 0 to 4. They are therefore out of 20 points:
-
4.36 for the classical preparation
-
5.73 for the A. Tomatis preparation
This first table therefore reveals an initial anxiety majored in the starting A. Tomatis group, expressing itself for example in mood disorders: worry, irritability, easy crying, apprehension, expectation of the worst.
-
1.21 for the classical preparation
-
1.54 for the A. Tomatis preparation
As for the other manifestations of this anxiety: in relation to intellectual functions, to cardiovascular, gastrointestinal disorders or insomnia, these nuances are not significant. One may only conclude that the starting groups have a homogeneous aspect. Let us now study the evolution of each of these groups by detailed items over the course of the preparation.
1 — Anxiety scale
The classical preparation group
The global average score of anxiety increases significantly at the end of preparation: 4.36 → 4.71.
This is observed in particular by an increase in sleep disorders, markedly accentuated: 0.83 → 1.47.
But cardiovascular symptoms and mood disorders are improved at the end of preparation. As for the disorders of intellectual functions or gastrointestinal symptoms, no significant modification is observed.
What are the traits particular to the evolution of the Alfred Tomatis Group?
-
The global benefit relative to the average anxiety score is a diminution of nearly two points in total: 5.73 → 3.95.
-
The areas most sensitive to this improvement: gastrointestinal disorders (score divided by two), cardiovascular symptoms, then mood disorders.
-
There is no notable change with respect to intellectual functions and no correction of sleep disorders (which express themselves little).
Analysis
The Alfred Tomatis method notably and globally diminishes the ANXIETY of pregnant women during the preparation, whereas in the starting group, this disorder was exacerbated. The classical preparation does not bring this benefit. One may think that the anxiety which increases significantly in women following a classical preparation is physiological, linked to the approach of childbirth, to the disorders majored at the end of pregnancy, expressing themselves, as we have seen, in insomnia. Without going so far as to think that the preparation generates this anguish… at least it is not apt to correct this disorder significantly.
INSOMNIA is a disorder noted with more intensity at the end of preparation in women having followed the classical courses, while in the A. Tomatis group, at an apparently homogeneous starting level (since without significant difference), this disorder is not modified. The A. Tomatis preparation therefore contributes to preventing an increase of the sleep disorder as it expresses itself in the other group.
In the two groups, one observes a significant diminution of MOOD disorders between the beginning and the end of preparation. Now, before the preparation, this item was notably majored in the A. Tomatis group relative to the classical preparation. This difference disappears at the end of preparation. The A. Tomatis method has therefore contributed to diminishing an anxiety which was majored at the start in the expression of mood disorders.
The expression of anxiety in GASTROINTESTINAL disorders is noted in a homogeneous way in the two groups before and after the preparation. However, the diminution is significant in the A. Tomatis group, probably therefore more conclusive as to the correction of these symptoms.
For CARDIOVASCULAR disorders, the diminution is significant in the two groups between the beginning and the end of preparation. Moreover, the groups are homogeneous at the start and arrival. One concludes that the two preparations are of the same effectiveness with respect to these symptoms.
As for INTELLECTUAL functions, the disorders would not be modified in one sense or the other, whatever the preparation. None of the figures is significant. One cannot therefore draw any conclusion.
Conclusion
In the main lines of this statistical study, according to the Hamilton scale, one will retain:
-
An average of anxiety stronger in the starting A. Tomatis group and a quite beneficial improvement relative to the classical preparation.
-
This plays in particular on sleep disorders which are not aggravated thanks to the phonic preparation.
-
For the other symptoms, one observes in the Tomatis group an improvement at least equivalent to the classical preparation.
2 — Testimonies
Postpartum or phrases heard in preparation sessions, we report here the key phrases of a dozen interviews in order to better understand what the phonic method seems to have brought them during pregnancy. These points are essentially subjective. They complete the analysis of the Hamilton scale which is purely objective.
The element that seems primordial to them is the very beneficial contribution of the preparation relative to SLEEP.
-
“The preparation helped me to recover sleep, to be less nervous.”
-
“I had few sleep problems, but there I slept ten times more.”
-
“After the sessions, I always took a long nap.”
They also underline the dual aspect of the work of the Electronic Ear on the person: the RELAXING and DYNAMISING side.
-
“For an hour, one is cool, it is very relaxing, these sessions. One comes out of them with the desire to move mountains.”
-
“I found it passive but it is very pleasant and dynamising.”
The atmosphere of the course is evoked in their testimonies. This reflects the importance of the role of the group: small number (12 persons), identical persons at each session, which allows the women to feel really at ease there. They all evolve at the same rhythm relative to a technique (unknown at the start). They evoke: the ease of discussion with the midwife or other women of the group at the end of the course. Madame Tordjman describes it as CONVIVIALITY:
-
“The atmosphere between these two preparation groups has nothing to do with each other. Perhaps the people are not the same? There are surely common points.”
-
“It is incontestable, something happens. To be well during the session is worth it even if there is only that.”
-
“One comes to the hospital in a different way. One chooses to come. It is neither for a course nor for a consultation.”
With this preparation, how did they approach childbirth, and what do they say about their birth a few days later?
-
The well-being they describe from these phonic sessions reverberated in daily life:
-
“I took the time to rest.”
-
“I let myself live.”
-
“I took the time to listen to music to relax.”
-
Their approach to childbirth seems interesting:
-
“I arrived, I was very cool, not anguished at all.”
-
“Either I was unconscious, or I was hyper-relaxed.”
-
Even if for the birth they say it did not help them at all:
-
“It changed nothing at all. I panicked like everyone else, but I do not at all blame the preparation.”
-
One notes interesting reactions which lead us to evoke the benefits of the rest and relaxation “stored up” during pregnancy:
-
“Six hours after the epidural, I had pain, it was very violent. I had no recourse. I tried to breathe well, to calm myself by saying: I absolutely must assume it.”
-
“A. Tomatis changed nothing in the respiration, in the pushing efforts, etc. The benefit is that one is more relaxed.”
Their way of being postpartum also seems imbued with the benefits of the sessions of the Alfred Tomatis method.
-
“I feel a little excited, but not tired. Still relaxed and not anguished about going home.”
-
“Sophrology had brought me more for childbirth, but there I do not feel exhausted as the first time.”
-
What to say of the beginnings of mother-child communication, except that it can only be favoured if the woman is rested, less anguished, and feels more dynamic?
-
“The fact of being more relaxed influences him.” Postpartum, they all say that their baby seems calm, with much reserve relative to the preparation sessions: “does it favour or not?”.
-
A “detail” representative of the impact of the preparation on the first signs of communication: during the sessions, the children react differently according to the music. Often, during the Gregorian chants (with their slow rhythm that mimics the calm, appeasing physiological rhythms), one notices that they move more. The mother is very relaxed and therefore very sensitive to these varying perceptions. She is fully attentive to the reactions of her baby.
Childbirth
Introduction
Preparation for birth according to the Alfred Tomatis method favours the well-being of the pregnant woman. The term psychological comfort then seems adapted. We have seen that beyond pregnancy, we may hope from it an appreciable repercussion on labour, on childbirth and on the newborn. We have based ourselves on a theoretical reasoning in broadening the fields of application of the Electronic Ear. Can we really speak of comfortable childbirth? Are the maternal and foetal risks diminished? The analysis of objective parameters qualifying births will allow us to respond to these two questions. We shall compare women prepared by the Electronic Ear, by classical courses and unprepared. We shall try to illustrate the percentages and averages with graphs. The figures are all compared according to recognised statistical methods (Chi-square test, the reduced difference of two averages). We shall study for these three groups of women:
A. Maternal surveillance
-
the mode of childbirth,
-
the motive of admission to the labour room and the mode of triggering,
-
duration of labour and other time parameters,
-
uterine dynamic,
-
pathology of labour,
-
anaesthesia
-
state of the perineum
B. Foetal surveillance
-
Gestational age,
-
foetal cardiac rhythm,
-
amniotic fluid,
-
presentation,
-
the child according to birth weight, Apgar, pH then the mode of feeding.
Thus we shall know whether the Electronic Ear, through a re-education of listening, acts on childbirth and on the general state of the child.
A. Maternal surveillance
1) Mode of childbirth
We distinguish 3 modes of childbirth:
-
spontaneous vaginal
-
non-spontaneous vaginal, therefore forced
-
caesarean
Whatever the classical and/or A. Tomatis preparation, the percentages of vaginal (55%), forceps (33%) or caesarean (12%) are considered statistically identical. But we observe fewer forceps for unprepared women (27% against 33%) and more caesareans (9% against 12%). The percentage of spontaneous vaginal remains identical to the two other groups: 54%. (Figure 10 in the annexes)
2) The motive of admission and the mode of triggering
Let us look at these two characteristics in order to understand the origin of these differences.
We distinguish 7 motives of admission. For the 3 groups, we note:
-
76% of spontaneous labour
-
4% of programmed triggering
-
3% of triggering for pathology
-
3% of caesareans at the start of labour
-
0% for post-partum
-
0% for transfer after caesarean (Table 11, annex)
For the A. Tomatis group, 23% of admissions take place for premature rupture of membranes against 12% for the other women, that is, twice as many. We observe no other significant difference. Do the premature ruptures of membranes entail a greater number of artificial triggerings?
The data show that there are 10% on average of artificial triggerings in the three groups. They are programmed, of convenience or on medical indication.
Women having followed an A. Tomatis preparation, who ruptured prematurely, therefore go into labour spontaneously without major complication of infection or foetal suffering… The case arising, a triggering on medical indication would have been envisaged. We do not observe an increase of artificial triggerings.
We may also remark that the rate of caesareans is twice as high in unprepared women: 4% against 1% and 2% for the other women. This difference is significant. We may suppose that:
-
Women who will have a first-intention caesarean do not see the necessity of a preparation for birth.
-
Or that women not enrolling in preparation courses are less well informed and/or less well followed. This would increase the risk of occurrence of a pathology of pregnancy (through the absence or scarcity of information), which would increase the risk of emergency caesarean at the start of labour.
Conclusion:
The preparation under the Electronic Ear seems to increase the risk of premature rupture of membranes, but it does not appear major since it does not require an artificial triggering.
-
The mode of childbirth is identical to women prepared by classical courses. The premature ruptures of membranes of these women therefore do not engender pathologies.
-
The prevention of caesareans and forceps is not improved by the Tomatis preparation.
3) Study of the time parameter:
-
Average duration of labour:
-
Without preparation 7h51 min (base 245)
-
Classical preparation 8h12 min (base 683)
-
A. Tomatis preparation 7h19 min (base 53)
According to statistical tests comparing averages, the labour of women prepared by A. Tomatis is significantly less long than the other women.
- Study by slice:
Only the percentages of women giving birth in less than three hours are significantly different between the three groups. 17% of women prepared by A. Tomatis give birth quickly against 15% of unprepared women and 6% of classically prepared women. But most women — more than half —, whatever their group, give birth between 4 and 8 hours and a quarter between nine and twelve hours (refer to the annexes, Figure 13)
- Duration of dilation between 5 cm and complete:
This phase of dilation lasts about three hours, equivalent average for the three groups.
- Duration of expulsive efforts:
The time is evaluated at fifteen minutes on average for all women. By studying by slices (less than fifteen minutes, from sixteen to thirty minutes, more than thirty minutes), we note that unprepared women are more numerous to have a short time of expulsion: 75% against 64% and 68% (64% and 68% are not significantly different).
Let us try to understand these figures:
By computer data, the percentages count all women, including those who have had a caesarean, which annuls their expulsive efforts. Now let us recall that there are more caesarean women in the group without preparation, whence a higher percentage for the group without preparation at short times of expulsive efforts.
The preceding figures indicate a higher rate of forceps in the two prepared groups relative to the group without preparation, which explains, without doubt, the higher percentage of women having a time of expulsion greater than 15 minutes for these two same groups.
Conclusion:
No element allows us to think that the A. Tomatis preparation influences the time of dilation and the duration of the expulsive effort. We just observe that the average duration of labour is slightly inferior to the other women. It reflects the more important rate of primiparas giving birth in less than 3 hours.
4) Study of the uterine dynamic
The uterine dynamic is studied on the qualitative plane (normal, hypokinesis, hyperkinesis, hypertonia) and on the existence or not of a stagnation of dilation — a reflection of its effectiveness.
More than 80% of women have a normal uterine dynamic. In the A. Tomatis group, we find twice fewer anomalies of the uterine dynamic: 8% against 15% in the two other groups. This difference is particularly notable on the rate of hypokinesis: four times less hypokinesis, that is 2% in women of the A. Tomatis group against 8% for the others. By contrast, this difference has no repercussion on the rate of dynamic dystocia: 13% of women, whatever their group, present an anomaly of dilation.
(Figure 14 in the annexes)
This may be explained by the use of oxytocics. We use SYNTOCINON before any anomaly of the uterine dynamic without waiting for a stagnation of dilation.
Conclusion:
The A. Tomatis preparation seems to favour the uterine dynamic. We may wonder if the term of childbirth (one week of difference with the classical group) and the lesser rate of prematurity do not play a role in the uterine dynamic. A second explanation may be proposed: premature rupture of membranes.
At 40-41 weeks of amenorrhoea with ruptured membranes, the conditions would be optimum for a good muscular work of the uterus. We do not unite here sufficient elements to confirm this supposition.
5) Study of the different pathologies of labour
Women prepared according to the Alfred Tomatis method complicated their labour with the following pathologies:
-
hyperthermia above 38°: 19%
-
acute foetal suffering: 4%
-
mechanical, cervical and/or dynamic dystocia: 19%
-
defect of progression at expulsion: 13%
-
defect of rotation at expulsion: 2%
-
pathological foetal cardiac rhythm at expulsion: 6%
We therefore only studied these pathologies in comparison with the two other groups. Other obstetric pathologies such as:
-
Failure of triggering,
-
shoulder dystocia,
-
maternal fatigue…
Are found in the unprepared groups or prepared by classical courses. They have not seemed interesting to mention here since they do not exist in the group prepared by the Electronic Ear. Let us underline some interesting figures: there are more hyperthermias in the A. Tomatis group: 19% against 11% for the two other groups.
Thanks to the computer data, we observe that hyperthermias are associated with mechanical dystocias: 2%, with dynamic dystocias: 2%. And with defects of progression at the expulsive effort: 9%.
87% of hyperthermias are isolated. The figures are identical for the two other groups. We do not find amniotic infection, foetal suffering, whereas they exist in the two other groups in an equivalent way. We must bring this figure closer to the 19% of premature ruptures of membranes, twice as frequent in the A. Tomatis group. Now, premature rupture and/or long labour linked to a dystocia are two factors favouring maternal fever. We may note that it is not major. It does not entail foetal suffering. It is not linked to amniotic infection. The prevention of infections is well effected.
Other elements brought to light
13% of defect of progression at expulsion against 22% for the two other groups. We do not have sufficient elements to explain this difference. We just note the absence of maternal fatigue in the A. Tomatis group. In the two other groups, it is figured at 3%. We content ourselves with raising the following question: does the Alfred Tomatis method help women during the expulsive phase, the only active phase of childbirth?
All pathology grouped
We notice that the frequency of pathologies during labour is identical in the three groups (refer to the annexes, Table 15) one woman in two, whatever the preparation effected or not during pregnancy, will have an anomaly of labour and/or of expulsion.
Conclusion:
If the frequency of pathologies during labour is identical, the type differs from a woman prepared by the classical method and unprepared to a woman prepared by the Alfred Tomatis method: more than 8% of fever and less than 11% of defect of progression for the A. Tomatis group.
6) Anaesthesia
Contemporary obstetrics is transformed by the frequency of childbirths under epidural anaesthesia. It brings irrefutable maternal comfort. The epidural is one of the first subjects evoked during the preparation course by patients. Do they influence the choice of women? Does the Alfred Tomatis method modify its frequency? What of other anaesthesias?
85% of women prepared by the Alfred Tomatis method and of unprepared women give birth with an anaesthesia and 90% of women prepared by the classical method. We observe two significant differences.
More than 5% of general anaesthesias.
Less than 11% of epidurals.
In unprepared women relative to women prepared classically (see Figure 16 in the annexes).
The two groups of prepared women (classical and A. Tomatis) do not present a significant difference. The differences noted are probably explained by caesareans. They are more readily effected under general anaesthesia for prepared women. This must be put in parallel with the pathological foetal cardiac rhythm, therefore the second-intention caesareans would take place more easily in an emergency monitoring not permitting the setting in place of an epidural catheter. Moreover, unprepared women have not received the explanations concerning the epidural during the courses. They do not know where the epidural can be done.
The reasoning does not allow concluding a connection between the A. Tomatis preparation and the choice of anaesthesia. The two prepared groups being homogeneous, we may think that the A. Tomatis preparation, on the same basis as the classical preparation, respects the choice of women as to their desire or not for an epidural. In any case, the Alfred Tomatis method does not go against this choice.
7) Perineum
The state of the perineum, that is, the necessity of an episiotomy at expulsion, is an element qualifying a childbirth. It may be due to a tense perineum, or to poor qualities of tissues. It may be effected according to the context:
-
prematurity
-
macrosomia hypotrophy
-
acute foetal sufferings
-
arrest of progression
It is therefore important to look for a possible relation between the preparation for birth and the existence or not of an episiotomy.
The prepared groups A. Tomatis and classical are homogeneous:
76% of episiotomies
24% without episiotomy of which
4% of simple tears
20% of intact perineums
(Figure 17 in the annexes)
We note a difference of 11% on the rate of episiotomies between unprepared and prepared groups.
67% of episiotomies
2% of simple tears
31% of intact perineums
There again, the higher rate of caesareans in this group doubtless partly explains this difference.
According to these figures, we may suppose that preparation for birth by the Alfred Tomatis method has no influence on the occurrence or not of an episiotomy. This supposition cannot be confirmed. The preparation/episiotomy relation could be the object of a reflection exceeding the framework of this work.
Foetal surveillance
1) Gestational age
Let us compare the gestational age of the births of the three groups of women;
-
according to the Alfred Tomatis method
-
according to the classical method
-
without preparation
The curves are quite evocative in themselves. We note that:
in the group without preparation, there are:
-
12% of prematurity
-
85% of births between 37 and 42 weeks of amenorrhoea,
-
of which 50% at 39-40 weeks of amenorrhoea,
-
18% at 41 weeks of amenorrhoea
-
3% of post-term.
in the classical preparation group, there are:
-
4% of prematurity
-
93% of full-term births
-
of which 56% at 39-40 weeks of amenorrhoea
-
20% at 41 weeks of amenorrhoea
-
3% of post-term.
in the Tomatis preparation group, there are:
-
2% of prematurity
-
98% of full-term births
-
of which 56% at 39-40 weeks of amenorrhoea
-
35% at 41 weeks of amenorrhoea
-
0% of post-term. (see Figure 18 in the annexes).
Women prepared by the classical method give birth earlier than women prepared by the Electronic Ear:
-
the 1st between 39-40 weeks of amenorrhoea
-
the 2nd between 40-41 weeks of amenorrhoea
As for premature births, the analysis of the curves confirms the percentages. (See Figure 19 in the annexes).
-
The risk of prematurity is low in the two groups of prepared women: 3%. It is clearly higher for unprepared women — nearly four times more: 12%. According to these figures, we may think that preparations for childbirth diminish the rate of prematurity. It must be underlined however that threatened premature births, treated with rest, contraindicate preparation courses. Women are therefore counted in the group without preparation.
-
The type of preparation does not seem to diminish or increase the risk of prematurity. We do not observe a significant difference between 2% and 4% according to the Chi-square test. We shall therefore retain that the Alfred Tomatis method brings nothing more relative to the classical method as to the prevention of prematurity.
Post-term.
3% of classically prepared and unprepared women give birth after 42 weeks of amenorrhoea. In the A. Tomatis group, we observe no post-term birth but statistically the figures do not present a significant difference. The risk of post-term is identical for all women.
2) Study of foetal cardiac rhythm
We qualify each foetal cardiac rhythm as normal, suspect or pathological by studying it during dilation and during expulsion.
- during dilation, the groups of prepared women
(classical preparations and A. Tomatis) are homogeneous:
-
62% normal
-
33% suspect
-
2% pathological
In the unprepared group, there are twice as many pathological rhythms, that is 5% against 2% in the other groups. This is counterbalanced by 25% of suspect rhythms against 33% in the other groups. We may relate the higher number of pathological rhythms to the rate of caesareans, there also more important relative to the two other prepared groups.
(See Figures 20 and 22 in the annexes).
during expulsion, for the three groups, there are:
-
4% of normal rhythms
-
73% of suspect rhythms
-
3% of pathological rhythms
-
20% are uninterpretable — not recorded or not qualifiable
-
The three groups are homogeneous (annex, Table 21)
Conclusion:
The A. Tomatis preparation does not seem to bring a new element relative to the classical preparation as to the prevention of acute foetal sufferings. The group of women without preparation appears more exposed to obstetric pathologies. Indeed we may establish a cause-and-effect relationship between prematurity, pathological foetal cardiac rhythm and caesareans. These three elements essentially differentiate the groups of unprepared and prepared women. We may therefore advance that preparations for birth act indirectly on the prevention of acute foetal sufferings by diminishing prematurity. Additional work would be necessary to confirm this hypothesis. But by this reasoning, we evidence that the A. Tomatis preparation has the same effect as the classical preparation.
3) Amniotic fluid
To compare this parameter between the three groups, we look at:
-
the modality of rupture
-
the quantity
-
the colour at rupture and at expulsion
Modality of rupture
The rupture of the membranes is effected according to different modes with the same frequency for the three groups. Statistically they are therefore homogeneous with:
-
61% of artificial rupture
-
26% of ruptures before admission
-
10% of spontaneous ruptures
-
3% of rupture during caesarean (Annex, Table 23)
We shall simply underline a higher percentage: 9% of ruptures during caesarean in the group without preparation. This is linked to the higher number of caesareans. We therefore observe less than two-thirds of artificial ruptures and more than one-third of spontaneous ruptures. Let us recall that we noted a rate twice as high of premature ruptures in the A. Tomatis group (23% of motives of admission against 12% for the other groups). But the table shows that there are as many spontaneous ruptures in the three groups.
The quantity of amniotic fluid
We find as many normal quantity, oligohydramnios, excess of fluid for the three groups (Annex, Table 24), that is:
-
95% of normal quantity
-
2% of oligohydramnios
-
3% of excess of fluid
We cannot therefore draw any conclusion between preparation by the Alfred Tomatis method and the quantity of amniotic fluid.
Study of the colour of amniotic fluid at rupture
Whether it is clear, meconial, bloody, tinted, the distribution is identical for the three groups:
-
86% of normal fluid
-
8% of tinted fluid
-
4% of meconial fluid
Let us see whether this distribution modifies itself at the end of labour. The evolution of the colour of amniotic fluid during labour is an element permitting the diagnosis of acute foetal sufferings. There again, we observe no significant difference between the three groups. We may therefore say that globally there are at the end of labour:
-
80% of clear fluid
-
9% of meconial fluid
-
10% of tinted fluid (Annex, Table 25)
By comparing the two data, at rupture and at the end of labour, we notice for the three groups that at the end of labour there are:
-
less than 5% of clear fluid
-
more than 5% of meconial fluid
-
more than 1% of tinted fluid (Annex, Table 26)
We do not evoke bloody fluids since they remain identical in the two groups: 2% for the group without preparation. Moreover, they are not significant. So: prepared or not, for women, the risks of tinted and meconial fluid are identical. The three groups evolve in the same way during labour.
4) The presentation
We do not note a significant difference between the three groups of women as to the types of presentation:
95% of vertex presentations
4% of breech
1% of dystocic presentations (Annex, Table 27)
We cannot therefore establish a link between the preparation and the presentation.
5) The child
Comparison of birth weights:
-
Group without preparation: 3,180, + or − 70 grams (4480 − 940)
-
Classical preparation group: 3,280, + or − 35 grams (4580 − 1150)
-
Tomatis preparation group: 3,410, + or − 90 grams (5000 − 2770)
-
The children of the group prepared with the Alfred Tomatis method have a higher birth weight: +130 grams relative to the classical group and +230 grams relative to the group without preparation. The differences of averages are significant.
-
Two elements may act indirectly on weights:
-
The more important prematurity in the unprepared group and lower weight.
-
The women of the A. Tomatis group give birth between 40 and 41 weeks of amenorrhoea.
-
Classically prepared women between 39 and 40 weeks of amenorrhoea. Now the weight gain of foetuses is important daily at the end of pregnancy.
Study of Apgars at 1 minute and at 5 minutes
- At 1 minute:
The prepared groups (classical and A. Tomatis) do not present a significant difference:
-
86% of Apgars greater than or equal to 8
-
11% between 4 and 8
-
3% less than 4
The children of unprepared women have a better Apgar at 1 minute.
90% greater than or equal to 8
1% less than 4 (Annex, Table 28)
- At 5 minutes:
We observe significant differences between the three groups:
the children are more numerous to have an Apgar greater than or equal to 9 at 5 minutes: 98% against 96% and 93% in the two other groups
there is still 1% of children of the unprepared group who are less than 4 in Apgar
7% of children of the classical group still have a bad Apgar at 5 minutes, between 4 and 8. The two other groups comprise only 2% of children. (Annex, Table 29)
Let us compare the Apgars at 5 minutes to those at 1 minute:
-
+7% for the classical and unprepared groups
-
+11% for the A. Tomatis group
-
1% of children of the unprepared group remain still with an Apgar less than 4 at the end of 5 minutes.
-
For an Apgar 4-8 at 5 minutes, we count a diminution of 5% of children relative to 1 minute for the unprepared and classical groups. By contrast, the A. Tomatis group counts 9% less. One passes from 11% to 2%. The children of an A. Tomatis group recover much better and more quickly than the other children.
Let us recall that the A. Tomatis group has a shorter labour than the two other groups, that the children have a higher birth weight and that it counts fewer prematurities. This may explain this observation.
Study of arterial pH at birth
We compare the arterial pH at birth of the children of the 53 women prepared by the A. Tomatis method to the global population of primiparas over the year 1991, that is, the groups of women prepared classically and without preparation.
-
For all, three-quarters of pH are greater than or equal to 7.20. So 73% have a good pH.
-
23% of moderate acidosis
-
6% of severe acidosis
Without statistically significant difference, we note however, for the A. Tomatis group, 11% of severe acidosis, that is more than 5% than the control group. We are surprised by this high figure. The study of the preceding parameters does not let it be foreseen and does not explain it. We propose therefore to look at the six cases in order to understand the origin of these acidoses and to appreciate their repercussion and neonatal evolution.
We find:
-
Two foetal sufferings for stagnation of the presentation in the middle part.
-
Two premature and prolonged ruptures with suspicion of infection not confirmed by the child’s bacteriological samples. They are associated with funicular anomalies (loose circular), of which a rapid labour of 1h30, with repercussion on Apgar 6-8-10.
-
One dynamic dystocia caesareanised at 5 cm.
-
A funicular anomaly with very short cord. Only metabolic acidosis among the six cases.
These pH anomalies are principally respiratory acidoses: five out of six, with good recovery — that is, a pH greater than or equal to 7.20 after monitoring in the first hours without repercussion on the Apgar. We shall report the cases to the parameters previously studied. (Figure 30 in the annexes)
Analysis of the six cases of severe acidosis
- The A. Tomatis group is more exposed to premature ruptures of membranes and to maternal hyperthermias during labour. Now, two premature and prolonged ruptures are found in the low pH but are not complicated by maternal fever.
As for stagnations of presentation and dynamic dystocias, the A. Tomatis group is less exposed than the two other groups. We cannot therefore affirm that a greater number of these pathologies entails neonatal respiratory acidoses in this A. Tomatis group relative to the two other groups.
It also seems to us that a significant number of low pH is expressed by funicular anomalies: three out of six. It would therefore be interesting to look for the frequency of these anomalies and to compare the repercussion in the three groups. This study would allow us to express objectively the higher figure of low pH in the A. Tomatis group. Currently, with the elements grouped in our study, we can only observe this datum.
- For moderate acidoses, we note 13% of cases for the A. Tomatis group against 23% for the control group. There again, this is not statistically significant.
We shall therefore retain that 11% of women prepared by the Alfred Tomatis method present a severe neonatal respiratory acidosis. It corrects itself in the first hours. It seems linked to premature and prolonged ruptures of membranes and to funicular anomalies. But we cannot affirm this hypothesis currently.
Feeding at discharge
Four modes of feeding are listed:
-
maternal feeding
-
mixed feeding
-
artificial feeding
-
special diet
-
77% against
-
60% for the unprepared group
-
65% for the classical preparation group
These percentages of maternal feeding for the unprepared and classical groups are considered statistically different.
3% of children of the classical and A. Tomatis groups benefit from a mixed feeding against 5% for the unprepared group. But this difference is not significant.
As for artificial feeding, 29% of the groups classically prepared and unprepared have this mode of feeding against 17% for the A. Tomatis group. This is significant.
5% of children of the unprepared group need a special dietary regime against 2% for the other groups. The differences between the three groups on the time of feeding are therefore effected on the artificial feedings and the special diets, to the benefit of maternal feedings for the A. Tomatis group (Annex, Table 31).
We shall therefore retain that parents following the A. Tomatis preparation prefer to breastfeed their children — but do the choice of A. Tomatis preparation and of breastfeeding correspond to one and the same tendency? Or does the A. Tomatis preparation influence the mode of feeding?
We cannot respond to these questions with these simple data. We are not surprised by the different rates between the three groups concerning special diets. They confirm the conclusion of the preceding parameters (premature, foetal suffering). The unprepared group is more exposed to obstetric pathologies, and therefore neonatal.
Conclusion
In order to investigate the impact of the method of audio-psycho-phonological preparation on childbirth and on the state of the child at birth, we have just studied the objective parameters that qualify them. The A. Tomatis group is compared to the group without preparation and to the classical preparation group.
If the A. Tomatis method does not improve the prevention of prematurity, it favours births between 40 and 41 weeks of amenorrhoea — that is, a term higher by one week relative to the other women. By contrast, we observe twice as many premature ruptures of membranes without influencing the frequency of artificial triggerings.
The average of the time of labour is shorter by forty-five minutes. It is essentially due to the higher number of women giving birth in less than three hours.
The uterine dynamic of these women is improved. We find four times less frequency of hypokinesis without there being a significant diminution of dynamic dystocias.
The comparative study of the pathologies of labour evidences a risk majored by 8% of maternal hyperthermias for the A. Tomatis group, but most remain isolated. Premature ruptures do not seem solely responsible for this difference. We note fewer defects of progression at expulsion.
The more advanced gestational age for women explains the higher birth weight (130 to 230 grams more).
According to the Apgar, we notice that the “A. Tomatis babies” recover more quickly and better than the other children. This is probably linked to the term, weight, duration of labour, premature rupture of membranes favouring pulmonary maturation. In counterpart, the pH show more severe acidoses but they remain respiratory and correct themselves rapidly.
By our study, the premature ruptures of membranes, the maternal fevers, and the acidoses are not or partially explained. We observe them.
The pathologies do not appear to have major repercussions. The absence of complications proves that adequate care has contributed to a good prevention.
We must wonder whether the biases existing in our study do not modify the results obtained.
Third part: Discussion
A. Is the Alfred Tomatis method satisfying?
B. Bias and criticisms
C. Proposals
We have presented in a 1st part the Alfred Tomatis method and its author. Then in a 2nd part, the study of three groups of preparation has allowed the rigorous and objective definition of which elements of pregnancy or childbirth were influenced by the preparation. According to this analysis, we can now in a third part see whether the method of phonic preparation is satisfying:
-
For the patients who followed it,
-
for Tomatis according to what he expected from it,
-
and finally for the medical body.
We shall then evoke biases and criticisms as limits of our study. Then we shall envisage proposals in order to improve this preparation at Foch for the year 1992, according to the observations studied.
I) The principal question that motivated this dissertation is the following:
“Is the Alfred Tomatis method satisfying?”
- Our study allows us to affirm that future mothers are globally very satisfied with it. The analysis of the Hamilton scale and the interviews carried out postpartum are two complementary means of appreciating it. They have allowed us to demonstrate the benefit of preparation during pregnancy.
One of the advantages of the Alfred Tomatis method that we wish to highlight is its NEUTRALITY both for patients and for midwives. By its original principle, one notes that the Electronic Ear does not require, like other preparations (sophrology, yoga…), a particular training, a certain mode of life, even an ideology. It is noted for instance that the preparation does not influence their decision regarding the epidural or breastfeeding. They say that these choices were “already made” or are “totally dissociated”. One also notes their reserve regarding the preparation. Postpartum, they say: “breastfeeding starts well, the baby seems calm, I feel in full
Form… it is perhaps the influence of the preparation, I don’t know?”. These reactions well illustrate the non-dependence relative to the Electronic Ear. The work effected on the ear necessarily requires a repetition of several sessions but in a determined period. This mechanism is then mastered by the person, who self-monitors thanks to a better listening, a more dynamic statics. The process maintains itself through the woman’s own voice. These “details” seem important to us for the respect of an individuality.
For a satisfying work on listening, the sessions under the Electronic Ear must necessarily be frequent and close together, over a certain period. This explains the organisation of the preparation: two weekly sessions for five weeks. This pace may seem constraining. It requires a significant availability and motivation on the part of patients. Those we met considered the problem before investing themselves in this complementary preparation. They do not feel it as such. They come responsibilised, conscious of the well-being these sessions procure them. Through these two hours they take to relax, they sense the stake of communication with the child. They are content to come thus to the hospital. The time factor is therefore a false problem to resolve initially.
- What then to say of this new use of the Electronic Ear relative to its inventor… except that he expected nothing from it? Through the diversity of his fields of application as well as his numerous clinical observations, Tomatis expected no proof of the benefits of his method. The stake of the Electronic Ear at Foch for Doctor Alfred Tomatis was:
-
On the one hand, the satisfaction of placing his method at the disposal of a new public
-
on the other, to realise it in a large obstetric centre allowed studying its impact in a rigorous and objective way.
Thus, he confronts his enthusiasm with the reticence of the medical body. Yet he hopes to obtain from this experimentation a development of the method by midwives and obstetricians. Thus the Foch CMC appears as a pilot centre, of reference, for the large maternities which would wish to invest in this new method of preparation.
Let us underline that the Tomatis listening centres propose sessions to pregnant women but they are not integrated into a preparation course. He places the future of this method in the hands of midwives and physicians.
- The medical team constitutes indeed the third term to satisfy. Their reservations constitute a quite rich requirement relative to an innovation in the domain of preparation for childbirth. One must therefore take account of them.
-
The principal criticism bears on an absence of proofs of effectiveness at the moment of childbirth. We have responded to this objection by the rigorous analysis of obstetric parameters. Certain elements are significantly different.
-
There then comes a dissatisfaction as to the numbers. 58 women followed the preparation for a maternity which performs more than 2000 births per year… The figure seems low. We shall evoke certain proposals on this subject in a following paragraph. But one must take account of the fact that the method has only been set up in January 1991 and that it was virtually unknown to the general public. On the other hand, this small number is the reflection of a fundamental element of the method: the importance that this preparation gives to individuality. The fixed small group structure, allowing conviviality, must in no case be modified. But the way in which it is set up is criticisable on certain aspects. We study this problem in the criticisms and proposals.
What were the initial motivations of the medical body in taking on the responsibility of this preparation?
- The principal objective was to realise an evaluation of this new method of preparation for childbirth.
The Alfred Tomatis method applied to pregnancy and birth was innovated in the service of Professor KLOPFENSTEIN, a maternity hospital in the east of France. It was necessary that a large obstetric centre establish a work of analysis and evaluation. The Foch CMC has responded to this objective.
Moreover, it complements the work realised at Vesoul and participates in an opening of this new preparation for birth to the general public.
- This preparation also responds to another concern raised by the medical team:
Numerous are the women who follow a classical preparation at the Foch CMC. They recognise the necessity of it for general information on pregnancy and the learning of respiration exercises for childbirth. They affirm that this preparation in a large group little influences their experience as a pregnant woman. Indeed, the groups are large. This imposes a didactic course. A certain aspect of the preparation is then occulted. It is therefore in terms of complementarity that the phonic preparation was initially envisaged. This choice gave the maternity of the Foch CMC an image of modernity with the concern of offering its patients an original and interesting preparation for birth. The proposal of the Alfred Tomatis method at Foch reflects a will to favour the first mother-child links. Indeed, during the sessions, future mothers are attentive to this initial communication. Moreover, its originality sensitises the team on this point.
This innovation has had a non-negligible media impact: “Parents Magazine”, “Antenne 2” and other press have come or shown interest in the subject. This is perhaps not unrelated to the 2013 births celebrated on 31 December 1991!
Conclusion
The Alfred Tomatis method studied at the Foch CMC in 1991, despite a small number, brings numerous satisfactions.
The patients evoke it with enthusiasm.
Doctor Alfred Tomatis sees an opening in the use of the Electronic Ear to a new public.
This rigorous work of analysis gives him concrete and objective elements that study the effectiveness, the impact of his method on pregnancy and childbirth.
Finally, the medical body may refer to this study for the evaluation of a new technique complementing the classical preparation for birth.
II) Bias and criticisms of our study
Our desire for rigour and objectivity has necessarily masked certain psychological aspects, certainly more subjective. They yet seem interesting to us. Let us take for example the Hamilton scale. It is only a small means to evaluate the psychological comfort that women appear to derive from it. It only studies anxiety. We may evoke some elements that we have subjectively perceived having to do with this “psychological comfort”:
-
The calm of the babies remarked by the mothers,
-
their well-being postpartum, without apprehension of the return home.
We must consider this study as imperfect since it reflects only one aspect of the Alfred Tomatis method. For example, the Hamilton scale only evaluates anxiety during pregnancy. This seems to us insufficient to reflect the psychological state of a pregnant woman. A complementary work could be proposed in this direction. Nevertheless, this objective study is necessary since pregnancy is a new field of application of the Electronic Ear. Rigorous results are expected.
However, the principal bias of this dissertation, caused by an insufficiency of numbers, does not allow us to give many significant figures concerning childbirth. For numerous parameters, we have not been able to draw a clear conclusion between:
-
An absence of difference between the groups
-
or a difference masked by the too low number.
The three groups, according to their numbers, are not comparable.
III) Proposals
From this limit in our work, we hope much for the continuation of the Alfred Tomatis method proposed at Foch as a complement to the classical preparation. This continuity seems to us necessary in order to realise a more complete assessment and to respond to the expectations of the medical team as to those of the A. Tomatis team.
Nevertheless, for a better satisfaction of patients, we have drawn from our study on the year 1991 some suggestions for 1992. We allow ourselves to state a few remarks:
-
The Electronic Ear is only used two hours per week for the same group of 12 persons, which contributes to considerably limiting the number and which seems little for such a sophisticated technique that is within the reach of all. It would be desirable to envisage more flexibility in order to respond to a certainly more numerous demand (since they have all proposed it to their acquaintances…). This would eventually require the training of a midwife.
-
In addition to this investment in time and personnel, we solicit an acquiescence on the part of the team for better information, ease of access and to allow this method to develop. The Foch CMC is a pilot centre. Other maternities will be able to refer to it.
-
Finally, in discussing with the women postpartum, we have noticed that they still had questions about the method or had not well grasped certain aspects:
-
the closely spaced sessions
-
the gap between the end of the sessions and childbirth…
One could envisage arranging at the end of the phonic session a time of free exchange.
-
That they may speak of what the Alfred Tomatis method brings them
-
to insist on certain points to help them integrate the nuances of the Tomatis preparation such as: the training, the role of the maternal voice which maintains the phenomenon.
Conclusion
The Electronic Ear, at the basis of the Alfred Tomatis method, is a sophisticated means of demonstrating the importance of a quality of listening. For Alfred Tomatis the scientist, this apparatus constitutes the culmination of his research in audiophonology.
For Alfred Tomatis the clinician, it is only the starting point of a gigantic advance in the therapeutic domain.
In the course of his observations and astonishments, he perceived that through the re-education of the ear, he touched the verticality of the subject and his psychological reactions. The stake is considerable since a better listening allows the giving back to the patient of a dynamism and a more affirmed voice. It is an opening to communication.
By extension of his works, Alfred Tomatis took interest in the genesis of communication in the Uterine Night. It is thus that, by paying particular attention to the sonic awakening of the foetus, the phonic preparation for childbirth was born.
The Electronic Ear allows pregnant women “to open and enrich” their ear in order to be more relaxed and full of vitality.
As one woman said postpartum: “the simplest thing I could offer my child was to be well rested”.
The theory is seductive, the technique original. What is the contribution of this study for the experimentation of the Electronic Ear in the preparation for birth carried out at the Foch CMC?
The elements brought to light may be grouped under the term: psychological comfort:
-
A diminution of anxiety during pregnancy,
-
a serene approach to childbirth,
-
the return home envisaged without apprehension postpartum.
In the objective parameters of childbirth, we have retained:
-
A higher term of childbirth,
-
a more rapid labour,
-
fewer defects of progression at expulsion.
As regards the children:
-
A higher weight,
-
a better recovery (according to the study of pH).
But these too arbitrary data hardly reflect the experience of a birth. It would be interesting to define other parameters to study the benefit of a preparation at the moment of birth.
What are the repercussions and how does the phenomenon obtained at the end of pregnancy under the Electronic Ear continue?
The stake of the Alfred Tomatis method, thanks to the maternal voice and the tonus engendered by the re-education of listening, is the enrichment of mother-child communication. The bearing of his discovery therefore far exceeds, for Alfred Tomatis, the few hours of preparation at the eighth month of pregnancy.
It would be fascinating to be able to realise a longitudinal study in order to observe the evolution of the in-utero communication of the foetus lulled by Mozart and the Gregorian chants.
What does it become after birth, during the first days at the maternity, then in the infant and the young child?
Figures from the original document
Diagrams and illustrations from the PDF facsimile of the original article.
Figure 1 — facsimile p. 5
Figure 2 — facsimile p. 7
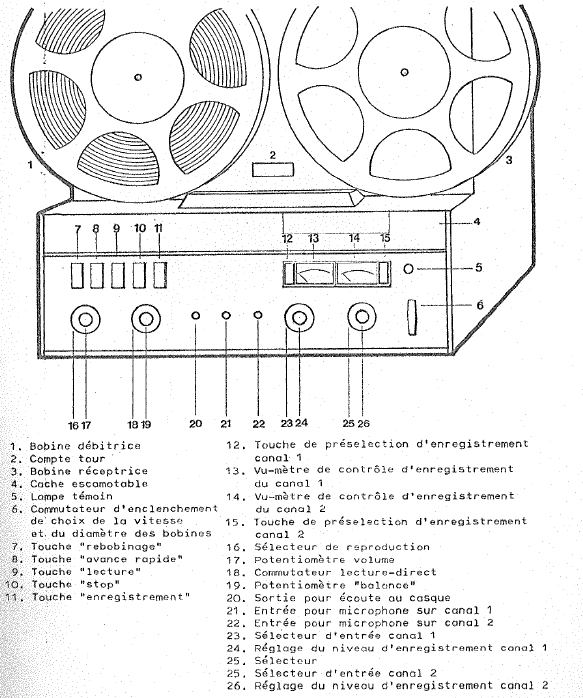
Figure 3 — facsimile p. 8
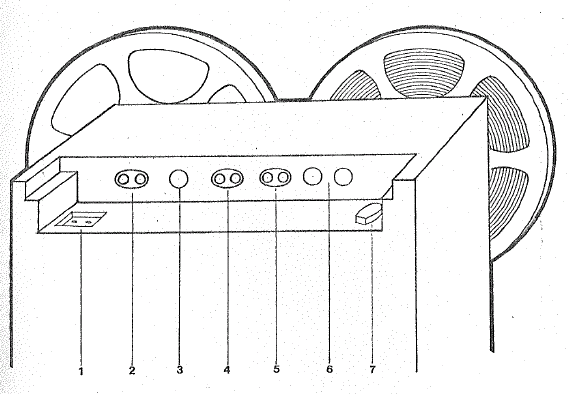
Figure 4 — facsimile p. 13
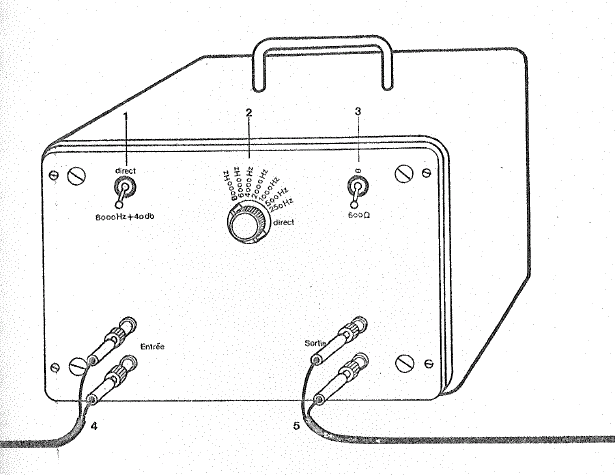
Figure 5 — facsimile p. 15
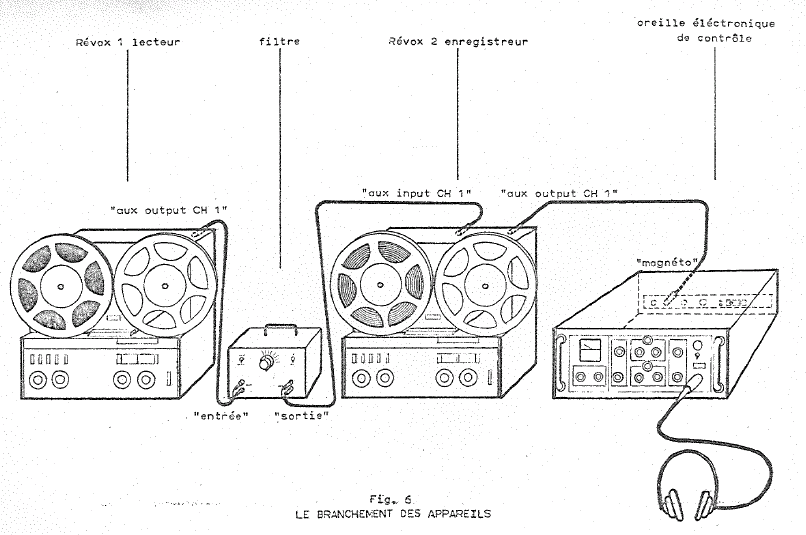
Figure 6 — facsimile p. 18
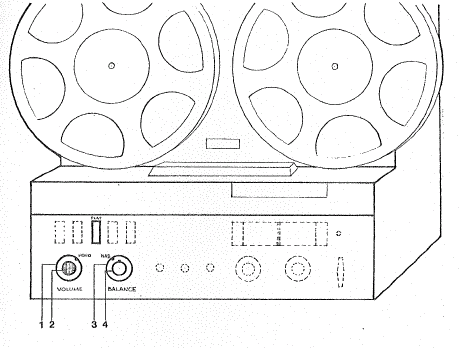
Figure 7 — facsimile p. 20
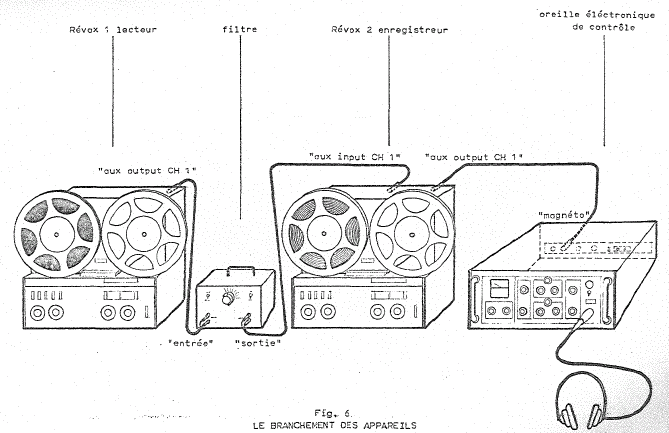
Figure 8 — facsimile p. 21
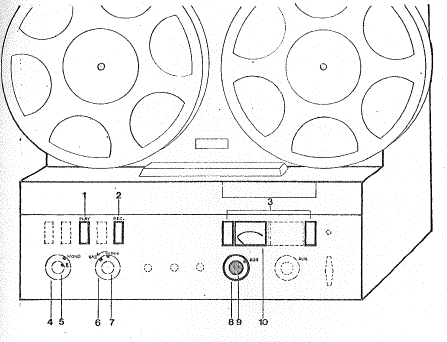
Figure 9 — facsimile p. 23
Figure 10 — facsimile p. 30