Objective Audiometry: Results of the Phonation-Audition Feedback
Objective Audiometry: results of the phonation-audition feedback — J.F.O.R.L. May-June 1957
Founding memoir by Dr Alfred Tomatis published in the Journal Français d’Oto-Rhino-Laryngologie, no. 3 — May-June 1957 (pp. 379-391). In thirteen pages and seventeen figures, the author establishes for the first time the concept of the directing ear — auditory analogue of the directing eye — and demonstrates experimentally the phonation-audition feedback. We find here: the dissociation between receptive musical ear and expressive musical ear, the identification of the transcerebral transfer (1/15th of a second) as the key to the pathogenesis of stammering, the demonstration of the occupational deafness of singers (intensities of 100 to 120 dB at one metre), the notion of auditory and vocal scotomata, then the description of the auditory selectivities proper to different languages (Italian, French, Russian). The text closes with the presentation of the objective audiometry apparatus with spectral analyser and white noise — the first instrumentation enabling the measurement of a subject’s hearing without his having to respond.
Extract from the Journal Français d’Oto-Rhino-Laryngologie
Number 3 — May-June 1957
R. Gauthier Printers, 35 Rue Viala — Lyon.
Objective audiometry: results of the phonation-audition feedback
Dr Alfred Tomatis (Paris) (*)
Introduction
The relations which make audition and phonation interdependent are so closely intertwined that the latter could not survive without the existence of audition — were it not for recourse to the artifice that is re-education.
To be sure, at first glance, this seems self-evident. However, as soon as one moves away from the prototypical case of the deaf-mute, the elements of this association appear less conclusive and demand more detailed analysis.
In the course of this exposition, we shall see that these relations are so closely linked in the phonation-audition direction that they constitute a true circuit, and any rupture, any tear, any anomaly, however minor, encountered in the circuit, is rapidly detectable.
-
Either because it brings about a disturbance in the rhythm, that is, a hindrance to the normal flow of the circuit;
-
Or because it allows a modification to appear in the timbre, that is, in the manner in which this flow takes place.
Disorders of rhythm. — The directing ear
In a previous work, we have evidenced the existence of an auricular predominance in the “aiming” of sound. There exists, in effect, a directing ear, just as there exists a directing eye in each individual.
This logical conclusion has proved easy to verify, and it is from the study of disorders of phonation in professional voice users that this suggestion arose, when we set about investigating the characteristics of the musical ear.
This directing ear is always lodged on the same side as the directing eye, that is, generally on the right in the right-handed person, on the left in the left-handed.
Its demonstration can readily be obtained by means of an apparatus that is easy to construct, composed of a microphone, an amplifier and a set of headphones. The subject sings into the microphone and listens to himself in the headphones. One can, at will, suppress the monitoring of one or other ear by means of a switch placing one of the two earpieces out of circuit, the one which remains in function being in parallel with a resistor of the same impedance as the eliminated earpiece.
We then observe that:
-
if the subject can monitor himself with both earpieces, he sings normally;
-
if one suppresses the left ear (the right ear having been identified as the directing ear), virtually no change is observed in the emission;
-
but if the subject sees his monitoring limited to his left ear, an immediate modification of the rhythm is observed in the direction of a very pronounced slowing, while at the same time the voice changes in timbre, becomes flat, white and loses its accuracy.
An experimental result of the same order is obtained if one disturbs the directing audition not by means of the small electronic device described above, but simply by inducing, for a few minutes, a dazzlement by white noise. The auditory fatigue, bearing only on the directing ear, allows the opposite ear a relative, non-permanent gain, which causes the same experimental disorders to appear.
The modification of rhythm can be considerable, for it has happened that we have obtained slowings exceeding, in duration, twice the duration of the melodic rhythm. This phenomenon is absolutely unconscious, and the forewarned subject must make a very considerable effort to make up this delay and sing in time.
The lack of accuracy is also a striking phenomenon. The monitoring of accuracy is, indeed, proper to the directing ear and calls upon, for this latter ear, audiometric characteristics that we have described elsewhere, and whose essential elements we briefly recall.
The audition of “musicians” in the broadest sense of the word, that is, of persons who have the capacity to hear and to reproduce accurately, presents an identical appearance in all of them, in the graph of measurements of auditory thresholds.
This curve always takes the form of that in figure 1, and a progressive ascent may be observed between 500 c/s and 2,000 c/s, with a difference in level varying, depending on the case, from 5 to 20 dB.
If this curve becomes dismembered, two phenomena then appear:
1° When the dismemberment occurs between 1,000 c/s and 2,000 c/s, as indicated in figure 2, the subject hears accurately but sings out of tune. He can sometimes become conscious of his shortcoming and succeed in correcting his deficiency in accuracy;
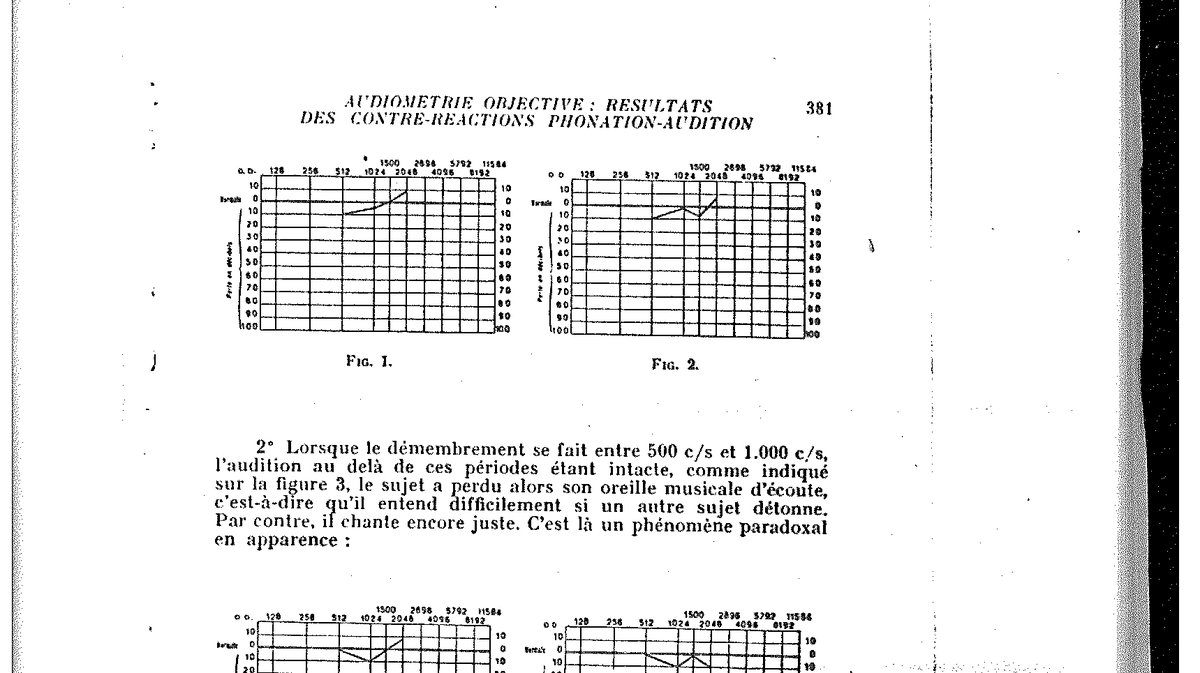
Fig. 1 and Fig. 2 — Reference audiograms: regular ascent from 500 to 2,000 c/s, difference in level of 5 to 20 dB; and dismemberment between 1,000 and 2,000 c/s.
2° When the dismemberment occurs between 500 c/s and 1,000 c/s, audition beyond these frequencies being intact, as indicated in figure 3, the subject has then lost his musical listening ear, that is, he has difficulty in hearing whether another subject sings out of tune. By contrast, he still sings accurately. This is an apparently paradoxical phenomenon:
3° Finally, if the dismemberment bears upon the whole curve, and if the latter no longer presents an ascending threshold limit and appears in jagged form (fig. 4), no character of musicality is found in the individual examined. He will hear and emit out of tune.
In sum, everything occurs as though there existed audiometrically a global musical ear capable of dissociating into receptive musical ear and expressive musical ear. But, a dominant fact, these characteristics have value only when applied to the directing ear.
If the opposite ear benefited from such advantages, the directing ear being deprived of them, in no case would we find in its possessor the characteristics of good musicality.
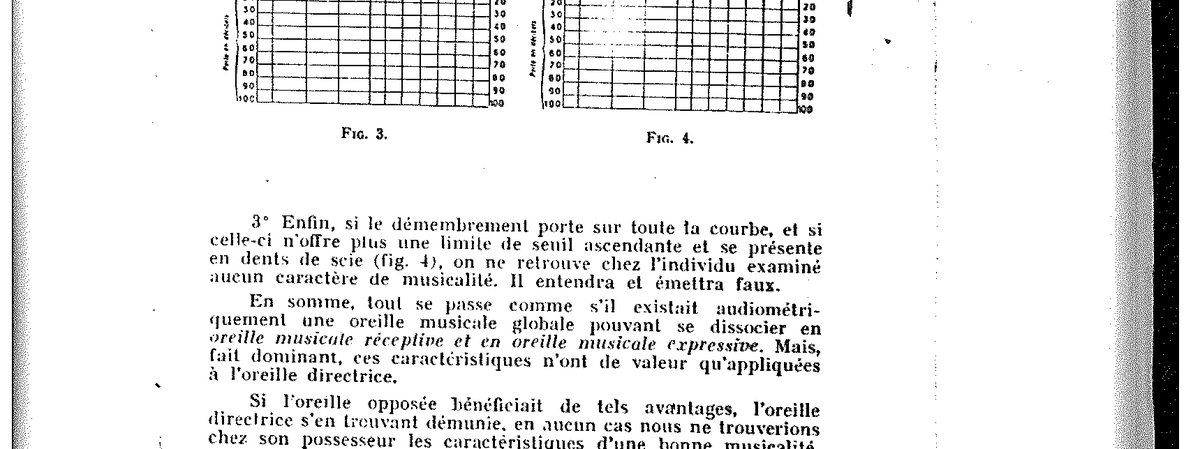
Fig. 3 and Fig. 4 — Audiometric dismemberment between 500 and 1,000 c/s; and total jagged dismemberment.
When the spoken voice — and no longer the sung voice — is considered, observing identical experimental conditions, one obtains even more precise responses.
Thus, upon the suppression of the directing ear, one notes, besides an immediate modification of timbre, disorders of rhythm more or less pronounced and variable depending on the individual examined, but specific and always identical for the same subject. One can then observe the whole gamut of anomalies of rhythm extending from simple stumbling to the most severe stammer.
This is a source of considerable research and a certain theoretical hypothesis on the pathogenesis of phonation disorders and, in particular, of stammering.
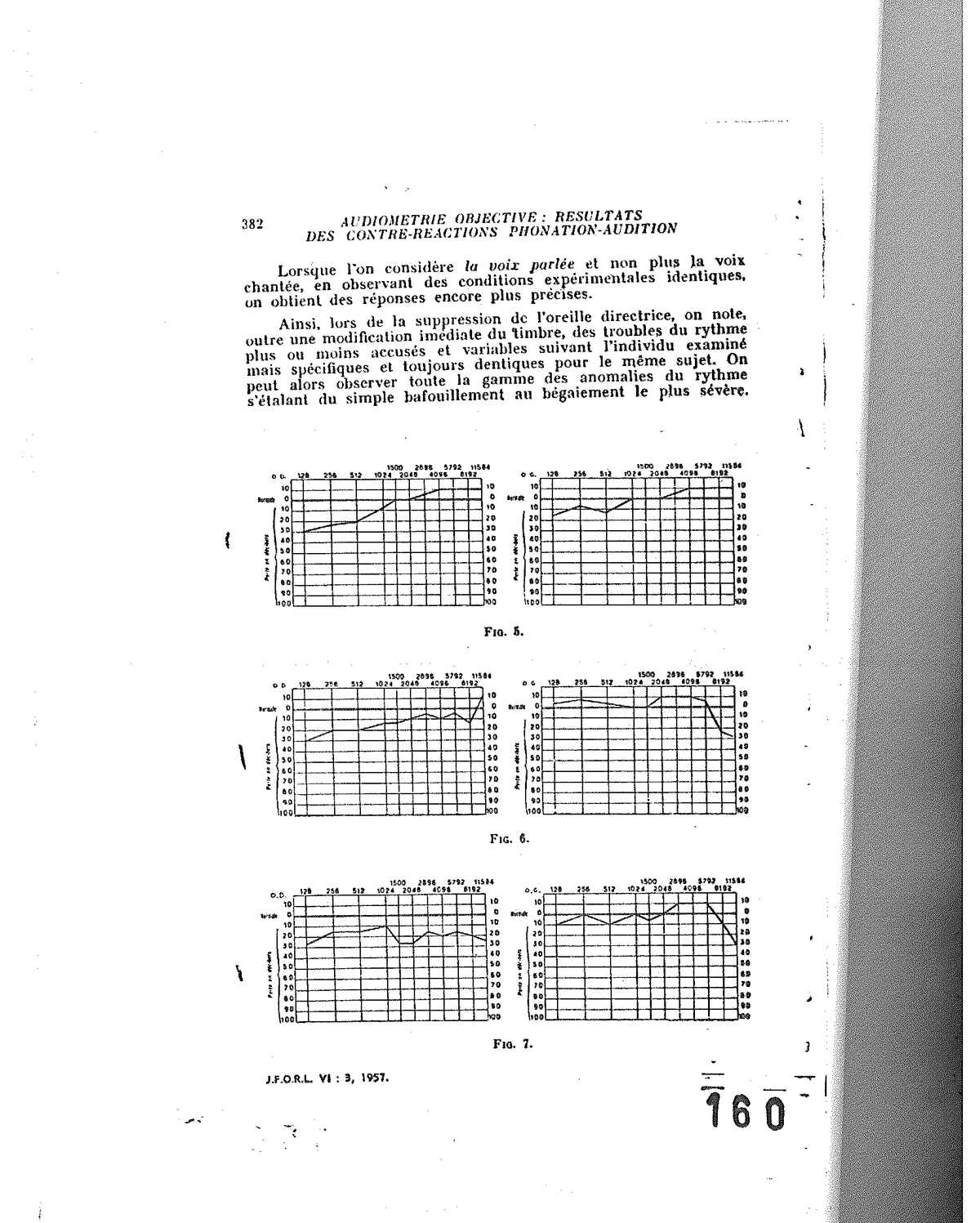
Fig. 5, Fig. 6 and Fig. 7 — Comparative audiometric series illustrating the anomalies of rhythm from simple stumbling to the most severe stammer.
Now, there is only a step to be taken to confirm this hypothesis by examining the audition of subjects afflicted with phonation disorders, notably stammerers.
This is what we have done systematically, and at present we possess some hundreds of audiometric observations. We reproduce here a few results, which we can divide into three groups.
The majority, at least 90%, corresponds to hypoacusic subjects of the directing ear.
As may be seen, this is only a relative hypoacusis, almost always unknown to the subject himself and detectable only at audiometry.
However, this hypoacusis is sufficient for experimentally, in suppressing the directing ear even in a partial way, one to obtain an identical result, as though a hypoacusis, however slight, of the directing ear sufficed to eliminate it from the circuit — the subject adopting straightaway the easy solution offered by the opposite ear, which benefits from a slight relative hyperacusis, but does not thereby become a directing ear.
We thus thought that we were faced with a profound modification of the audition-phonation circuit, and that it was in this disturbance that we were likely to find the explanation of the whole of the rhythm disorders.
We can readily evidence this anomaly on two very simple diagrams.
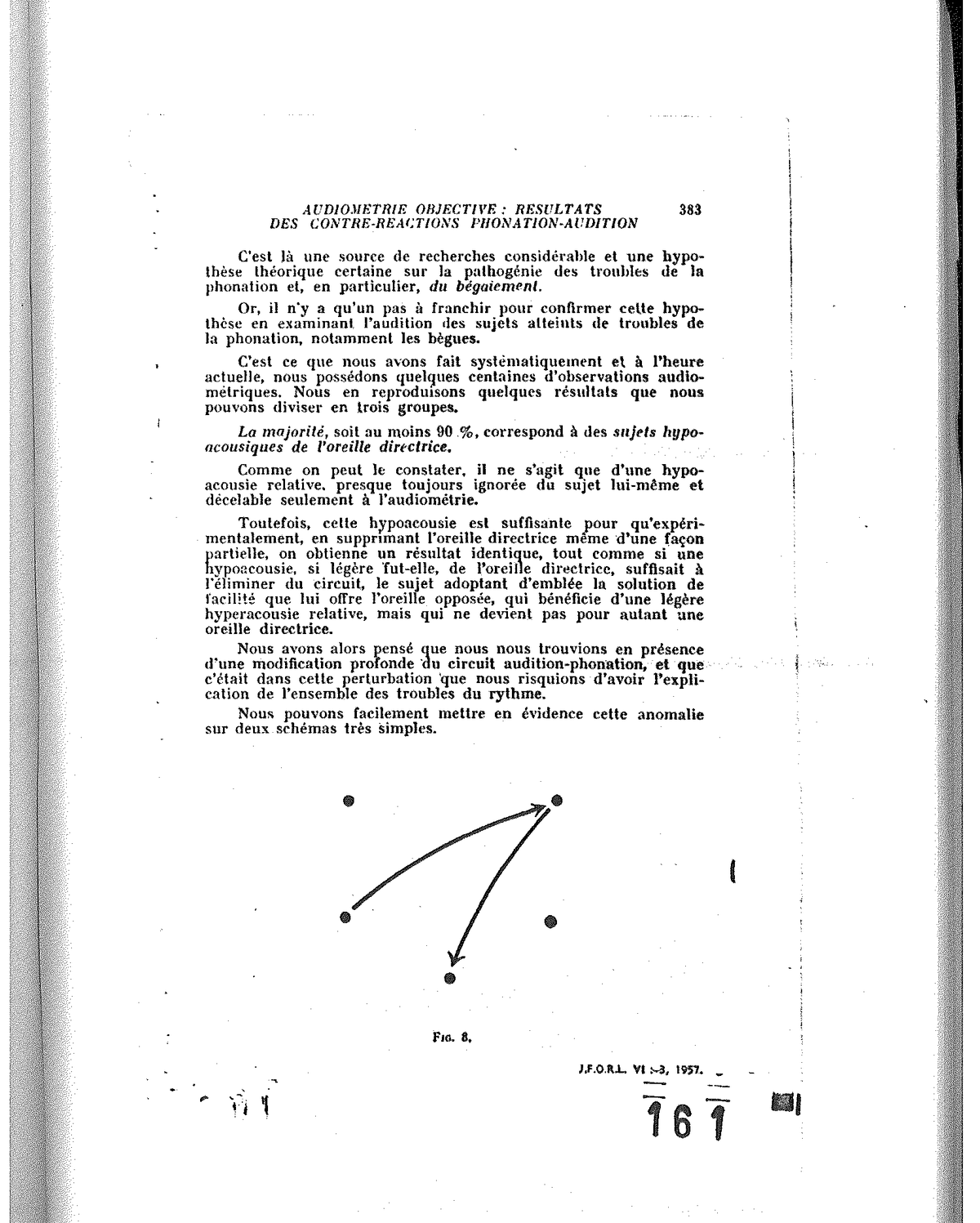
Fig. 8 — Normal route of the audition-phonation circuit: directing ear → left auditory centre → left motor centre → phonation musculature → mouth-to-directing-ear aerial route.
Normally, the audition-phonation circuit uses the following route (fig. 8):
-
directing ear (which we shall assume to be the right ear to simplify the exposition);
-
left auditory centre;
-
left motor centre;
-
phonation musculature;
-
and mouth-to-directing-ear aerial route.
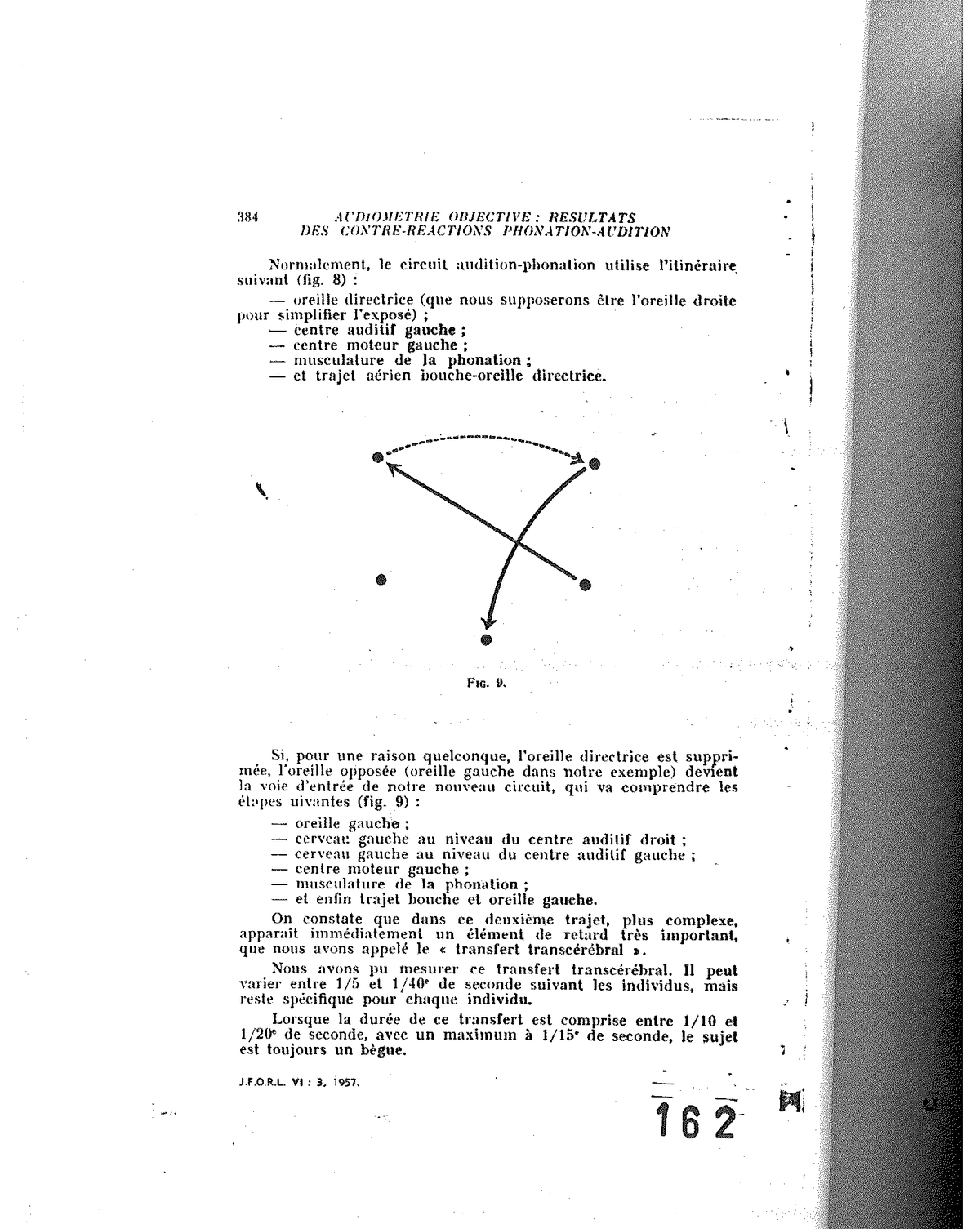
Fig. 9 — Disturbed route after suppression of the directing ear: the entry pathway passes through the opposite ear and requires an additional transcerebral transfer.
If, for any reason, the directing ear is suppressed, the opposite ear (left ear in our example) becomes the entry pathway of our new circuit, which will comprise the following stages (fig. 9):
-
left ear;
-
left brain at the level of the right auditory centre;
-
left brain at the level of the left auditory centre;
-
left motor centre;
-
phonation musculature;
-
and finally the mouth-to-left-ear route.
It will be observed that in this second, more complex route, there immediately appears a very significant element of delay, which we have called the “transcerebral transfer”.
We have been able to measure this transcerebral transfer. It can vary between 1/5 and 1/40th of a second depending on the individual, but remains specific for each individual.
When the duration of this transfer is between 1/10 and 1/20th of a second, with a maximum at 1/15th of a second, the subject is always a stammerer.
It is thus seen that not all individuals are necessarily stammerers if their directing audition is compromised. Two conditions prove indispensable:
-
the loss of the directing audition;
-
a transcerebral transfer of the order of 1/15th of a second.
Now, 1/15th of a second is roughly the average duration of the French syllable. Hence one understands better, on the one hand, the doubling of the syllable to recover this delay and, on the other, the phenomenon of repetitions which escapes the monitoring of the left cortex.
This value of 1/15th of a second, almost specific to stammering, explains the disappearance of the stumble when one imposes a slowing of speech, either artificially by imposing a bradylalia (*), or normally in all forms of language that increase the rhythm in duration, as is the case with the sung phrase.
It is also in the constancy of this value of 1/15th of a second that one can see a subject stammer in French and not in English, for example, the average value of the English syllable being 1/20th of a second.
It should be noted, in passing, that the delivery of a narrative learned by heart is performed without difficulty in the stammerer, for the command of phonation is made directly without the need for auditory monitoring.
Beyond these fortunately quite elective limits, the delays due to transcerebral transfer will be blocked by “ums” of greater or lesser duration, which repeat at intervals more or less distant, or by a more or less pronounced bradylalia.
In sum, this delay constitutes a true physiological “delayed feedback”.
Clinically the acute phonation disorders encountered in subjects afflicted with acute otitis affecting the directing ear come to reinforce this hypothesis.
For our part, we have observed two significant stammers during otitis — disorders which were to disappear as the directing ear resumed its functions.
One can grasp, in passing, the danger of an auditory loss on the directing ear, whether attributable to insufficient care, or consequent upon traumatising acts such as paracenteses.
The most important element, if not the proof, that has made us favour this hypothesis is the almost immediate disappearance of all phonatory disorders upon the restoration of the normal circuit. We use this regularly with success in the treatment of stammering.
Alongside these cases linked to a relative hypoacusis and representing 90% of the cases, there exist a certain number that simple audiometry does not allow to be detected, but which have a significant disorder of auditory selectivity. We shall have to return to this further on.
Finally, a third group brings together the subjects whose right-handedness is not evident, as in the bidextrous. The directing ear is then less clearly defined.
Disorders of timbre
a) Occupational deafness of singers.
It is again to professional voice users, notably singers, that we owe having thought of the possibility of a sonic self-trauma, after having analysed quantitatively the voices of all the singers examined.
The magnitude of the sonic energy they can deploy did not fail to surprise us, the more so as we had set out from classical but mistaken data, limiting the maxima to intensities of the order of 80 dB. Now, at one metre — the distance we have adopted as a reference — we have readily encountered 100, 110 and as much as 120 dB.
It is logical to think that an individual exposed to such an intensity for several hours a day might see a traumatic deafness install itself at the end of a more or less long time.
We here report a few typical cases that we compare with those of workers working near aircraft engines for an equivalent duration.
They can illustrate, both alike, as may be seen, the four stages of occupational deafness (figs. 10, 11, 12 and 13).
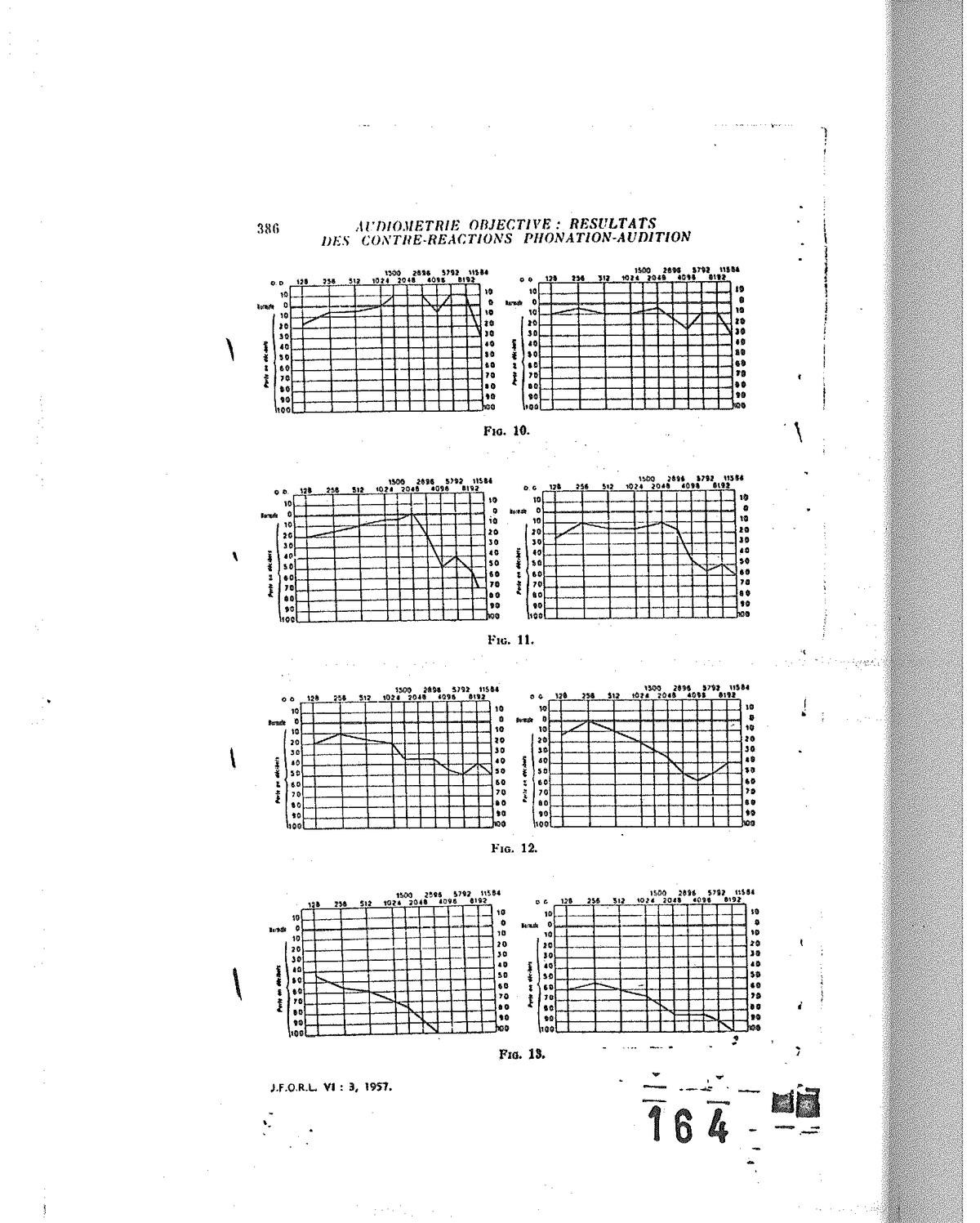
Fig. 10 to Fig. 13 — Four stages of occupational deafness, comparing singers and aircraft-engine workers; onset at 4,000 c/s and then extension towards high and low frequencies.
It is observed that in these singers, a deafness sets in, of the occupational deafness type, starting at the 4,000 c/s frequency and extending thereafter towards high frequencies, then low — exactly as in subjects exposed to noise.
In other words, and we insist particularly on this point, singers destroy their audition by their own sonic intensity — a phenomenon whose consequences are very grave.
b) Auditory scotomata (*) and vocal scotomata.
Indeed, the consequences are grave, for this auditory loss bearing selectively on high frequencies translates into a V-shaped scotoma that grows more pronounced, as we are accustomed to observe in occupational deafness — while disorders of the voice appear elsewhere.
To identify these latter disorders, we have practised a spectral analysis by sweeping a cathode-ray tube describing the frequencies on the abscissae and their relative intensity on the ordinates. Very rapidly we noted a fundamental phenomenon: the auditory scotoma translates into the appearance of a scotoma on the vocal spectrum.
We can deduce that the destruction of a voice is not linked, as is believed, to a wearing-out, to a destruction of the larynx, but to a diminution of the auditory field — the phenomena of laryngeal suffering being secondary.
Indeed, for a singer to obtain that high resonance he is ceaselessly seeking, he must absolutely have a perfect audition of the band extending beyond 2,000 c/s. As soon as he loses this possibility, his voice “passes into the throat”, and so-called laryngeal sounds are pushed and forced. At the outset, the singer uses resonantial possibilities — that is, standing waves easy to sustain without considerable muscular energy. By contrast, throat sounds, with strong laryngeal support, demand a significant physical expenditure and prove traumatising for the larynx.
The progressive loss of audition of high frequencies entails disorders of emission, all the more rapidly as the register requires the use of elevated ranges. Thus, tenors are the first affected, and as soon as the scotoma reaches 2,000 c/s, the singer’s career is seriously compromised. By contrast, it is known that a voice benefits from a duration all the longer as it is lower. Nonetheless it is less rich in high harmonics, it is whiter.
Without dwelling particularly on singers, one may readily note that the voice deepens as presbyacusis advances — in other words, as the individual ages.
In summary, one can say that a subject emits only the sounds he is capable of hearing.
Auditory selectivity
This last conclusion is still too broad and deserves to be examined. If it is true that an individual no longer reproduces the sounds he no longer hears, he does not, for all that, reproduce all those he hears.
This is why we have investigated what we have called auditory selectivity — that is, the capacity of an ear to perceive a variation of frequency within the sonic spectrum and to locate the direction of the variation.
We have used the following research procedures:
-
either by passing sounds going from high to low frequencies, and asking the individual from when the sound changes;
-
or by sending two sounds at variable intervals and at different pitches;
-
better still, by offering the subject, by means of a series of filters, the choice of adjusting his preferred mode of audition himself.
We then obtained surprising results as regards their theoretical import.
Indeed, in terms of auditory selectivity, there exists a well-defined ear for tenors, for baritones and for basses, from which emanates a theory of the registers that corroborates the earlier results.
Furthermore, there exists a racial audition on which we cannot, alas, dwell at length, but to which we hope to return shortly.
A few examples will suffice to show the full bearing of these phenomena.
The Italian ear is a very poor ear. Its selectivity lies between 2,000 and 4,000 c/s (fig. 14). It is null between 1,000 and 2,000 c/s, whereas the French ear is, by contrast, very limited between 1,000 and 2,000 c/s (fig. 15). We shall see experimentally the consequences. For example, the extraordinary appearance of the nasals as regards the French ear.
The Russians, by contrast, have a very extended selectivity, with a greater affinity towards low frequencies (fig. 16). Their voice is broad and warm. Moreover, this very extensive auditory band, contrary to the case of the French and the Italians, allows them to perceive all the consonants and, in consequence, to register them. It is known, indeed, with what ease Russians learn foreign languages. This phenomenon is due simply to their great auditory permeability.
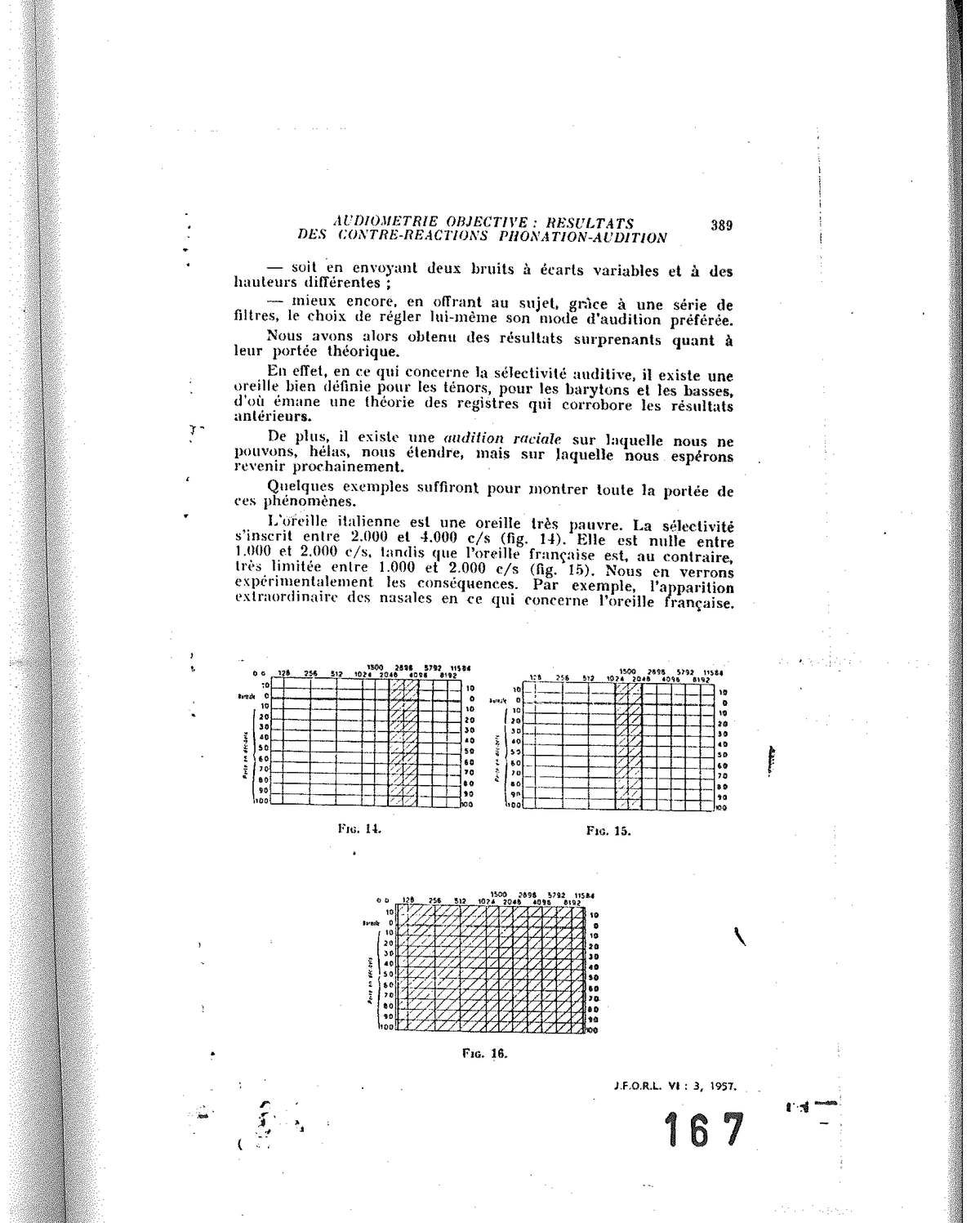
Fig. 14, Fig. 15 and Fig. 16 — Comparative auditory selectivity: Italian ear (2,000-4,000 c/s), French ear (very limited 1,000-2,000 c/s), Russian ear (very extended, affinity towards low frequencies).
Conclusion. — Objective audiometry
From these theoretical and experimental data, considerable practical elements may be drawn. Indeed, we have studied, for more than a year, an objective audiometry, without real participation of the subject examined, without one having to concern oneself with his responses. It is based solely on the preceding experimental observations.
Here is how we proceed:
The subject is placed before a microphone (M) as shown in figure 17. This microphone is connected to an analyser (An) with ultra-rapid automatic sweep and very extended band thanks to a superposition of five lines, allowing the spectral analysis of the sound from 0 to 10,000 c/s or 20,000 c/s over 50 cm.
This same microphone then allows the driving of an amplifier (Am), and several pathways are then offered to us:
1° By route I, the individual immediately receives his normal voice and can thus monitor it;
2° By route II, the amplified voice can, on command, pass:
-
either through a low-pass filter, variable from infinity to zero;
-
or through a band-pass filter, variable in spread and in height;
3° By route III finally, the voice is mixed with a background noise, white-noise type, which can be dosed in intensity (in decibels) and, in addition, limited in its dimensions of spread through the use of the low-pass, high-pass and band-pass filters.
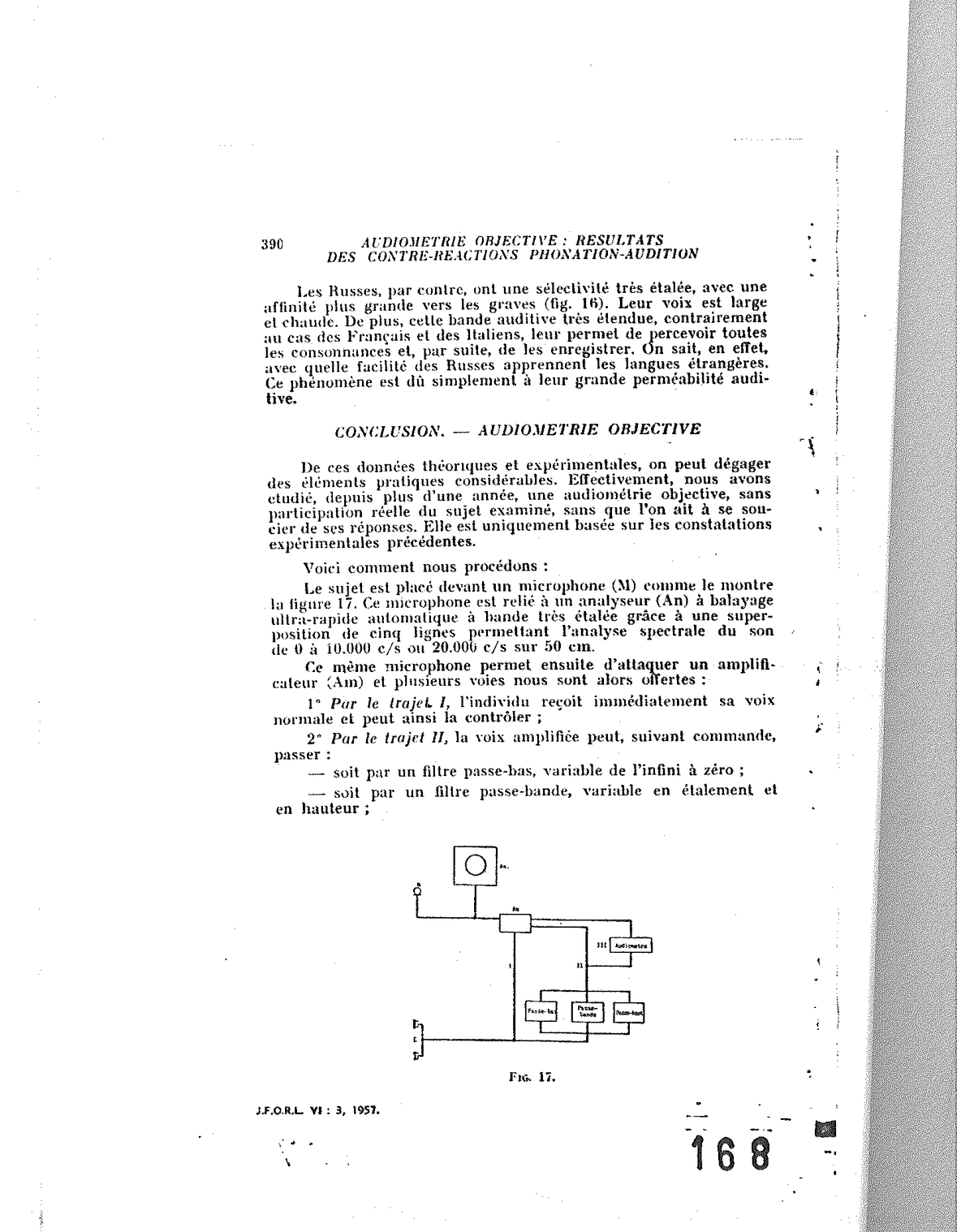
Fig. 17 — Diagram of the objective audiometry apparatus: microphone (M) → analyser (An) with ultra-rapid sweep → amplifier (Am) → three routes: I (direct return), II (low-pass / band-pass filters), III (filtered white-noise mix) → audiometer.
We thus obtain the following results:
1° By route I, the individual speaks normally into the microphone, monitoring himself by means of the earphones. We then obtain an envelope spectrum and we have seen that experimentally this spectrum is inscribed within the envelope curve of the individual’s auditory spectrum;
2° By route II, in using the low-pass filter, we cut all the highs at a variable height and we observe the compression of the sonic spectrum within the imposed limits. Likewise for the high-pass filter. In both cases, it is noted that, for certain zones, the individual no longer manages to saturate the bands offered. We are then in a zone he no longer perceives. Finally, thanks to the pass band that one can reduce or open at will and which one can slide over the whole route of the normal auditory spectrum, it is observed that the vocal spectrum follows the same pass band imposed on audition and, each time a gap reveals itself on the sonic spectrum of the cathode-ray tube, we find the auditory gap. This result always confirms the preceding one.
3° By route III, one can obtain another test by means of the white-noise generator. One sends, into the subject’s audition, a progressive background noise. At a given moment, it is observed that the vocal spectrum increases in intensity, and this in a global manner for all frequencies. We have then reached the threshold of audition. From this moment on, the subject speaks louder, but always presents a vocal spectrum of identical appearance — that is, without modification of timbre. One then increases a part of the spectrum of the white noise injected, bearing for example on the 0-1,000 c/s band. One sees the vocal spectrum make a translation towards high frequencies. The individual begins to speak louder and to change in timbre. This is a positive Lombard phenomenon.
We can then progressively spread our injected spectrum towards the highs. Beyond a certain limit, 4,000 c/s for example, the individual is incapable of going beyond it. At this point, we are at the upper limit of his audition of high frequencies.
One can thus know, without the subject’s awareness, the spread of his audition and produce a true objective audiometry, by audition-phonation feedback.
The few lines of this exposition show, therefore, the essential part that audition plays in phonation, and the important consequences of these relations, which we have only been able to summarise in this article.
(*) 78 avenue Raymond-Poincaré, Paris (16th).
(*) Bradylalia: slowing of speech.
(*) Scotomata: gaps.
Source: Tomatis A., “Audiométrie objective : résultats des contre-réactions phonation-audition”, extract from the Journal Français d’Oto-Rhino-Laryngologie (J.F.O.R.L.), vol. VI, no. 3, May-June 1957, pp. 379-391 (thirteen pages, seventeen figures). R. Gauthier Printers, 35 rue Viala — Lyon. Digitised document from Alfred Tomatis’s personal archives.