The Correction of the Sung Voice
The Correction of the Sung Voice — S.F.E.C.M.A.S.
Communication by Alfred Tomatis — then Ex-Assistant of the ENT Service of the Hôpital Bichat and Deputy Director of the Research Laboratory of the S.F.E.C.M.A.S. (Société Française d’Étude et de Construction de Matériel Aéronautique Spécial, Arsenal de l’Aéronautique). This nineteen-page memoir, preserved as an offprint (pp. 335 to 353), sets out the Tomatisian method for correcting the sung voice: the place of the phoniatrician between the ENT specialist and singing teachers, a fourfold examination protocol (otorhinolaryngological, magnetic recording, oscillographic-spectrographic analysis, audiometry), syndrome of auditory incompatibility between master and pupil, and the spectrographic demonstration of the vocal decline of Enrico Caruso from 1901 to the end of his career (Figs. 7 to 17). The author ends with the description of the re-education apparatus with low-pass / high-pass filters (Fig. 29), which constitutes one of the first public formulations of the Electronic Ear.
The correction of the sung voice
by A. Tomatis
Ex-Assistant of the ENT Service of the Hôpital Bichat,
Deputy Director of the Research Laboratory of the S.F.E.C.M.A.S.
Offprint, pp. 335-353 (nineteen pages, thirty figures).
I. — The phoniatrician, between the ENT specialist and the singing master
The examination of the sung voice, and still more its correction, obliges the phoniatrician to stand at the precise point where two universes meet: that of the otorhinolaryngologist, who looks at the larynx, and that of the singing teacher, who listens to its aesthetic result. It is in this frontier zone, long poorly inhabited, that we have sought to establish an objective discipline, capable of resting upon measurements and not only upon the impression — were it that of a very experienced master.
II. — How do we proceed?
Four complementary examinations constitute our protocol:
1° A complete otorhinolaryngological examination, with particular attention to the larynx, pharynx and nasal fossae;
2° A recording of the voice on magnetic tape, which will be the archive enabling later comparison;
3° An oscillographic and spectrographic analysis of each sound emitted, which delivers the harmonic envelope and allows comparison of the voice examined with the reference curves;
4° Tonal and vocal audiometry, supplemented by the study of the discomfort threshold and, when the nature of the dysphonia so justifies, by the discrimination tests.
III. — What do we see?
Two clinical pictures emerge with such regularity that we find them at every stage of our consultation:
A) The young subject in full vocal technique, who complains of an incipient dysphonia, a loss of accuracy, or an incapacity to cross a certain register.
B) The established singer, sometimes famous, whose great voice is crumbling and who sees his repertoire shrink.
IV. — A) The young subject in vocal technique
In this subject, two mechanisms are ordinarily encountered:
1° A rupture of synergy between respiration, laryngeal conduct and auditory monitoring. The voice slips, the emission becomes unstable, the ear can no longer bring phonation back to its habitual channel.
2° A syndrome of auditory incompatibility between teacher and pupil. This is an observation we have made on several occasions and which is admirably illustrated by the following case: a singer of twenty-four, in great difficulty with his master, came to consult us; his audiogram was identical to that of his teacher — an audiogram of the type we have qualified as a Caruso ear. The master’s technique, perfectly adapted to his own curve, became inapplicable to the pupil as soon as one sought to impose upon him an emission foreign to his audition.
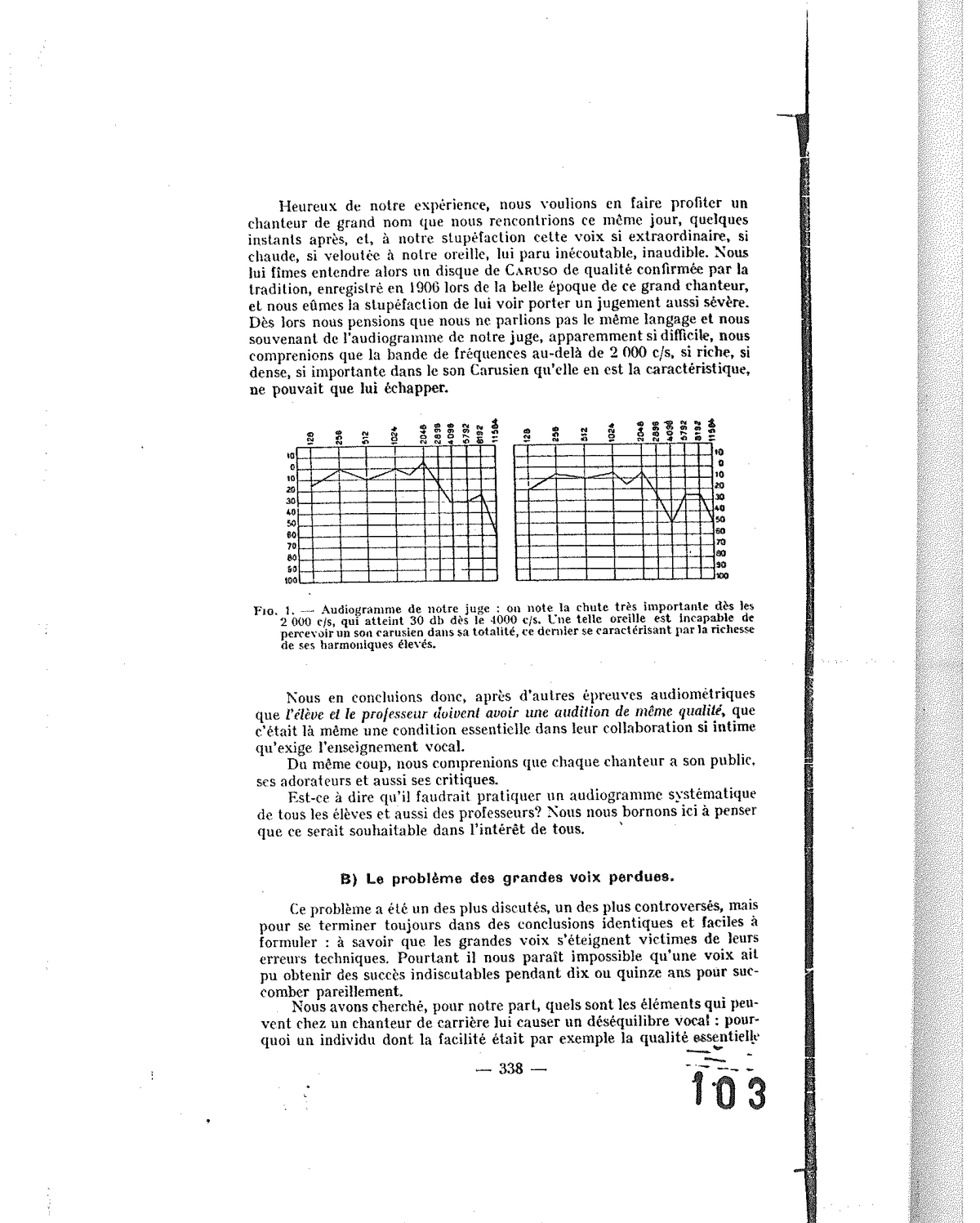
Fig. 1 — Audiogram of our judge: the very pronounced fall from 2,000 c/s onwards reaches 30 dB by 4,000 c/s. Such an ear is incapable of perceiving a Carusian sound in its totality.
From this observation flows a practical rule: it is important that the pupil hear approximately as his master does; otherwise, the master cannot transmit his vocal gesture without damaging the pupil.
V. — B) The problem of great voices lost
The second picture is that of singers in mid-career who see their voice deteriorate. Our audiograms almost always evidence an impairment of the reserve potential situated between 1,500 and 2,000 c/s — an impairment which corresponds to a prolonged exposure to high sonic intensities: the operatic voice, in full emission, reaches 110 to 120 dB at one metre from the vocal cords — a level largely sufficient to engender in the singer himself a true occupational deafness (Fig. 5).
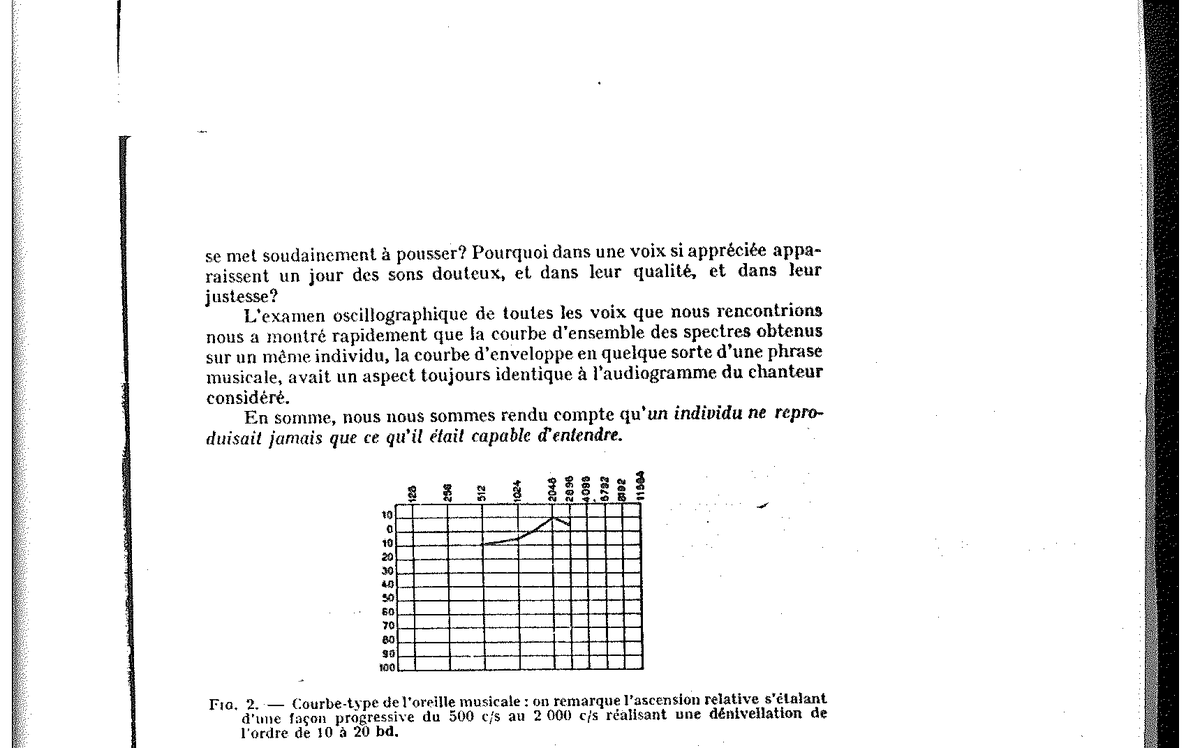
Fig. 2 — Type curve of the musical ear: relative ascent spreading progressively from 500 c/s to 2,000 c/s, difference in level of 10 to 20 dB.
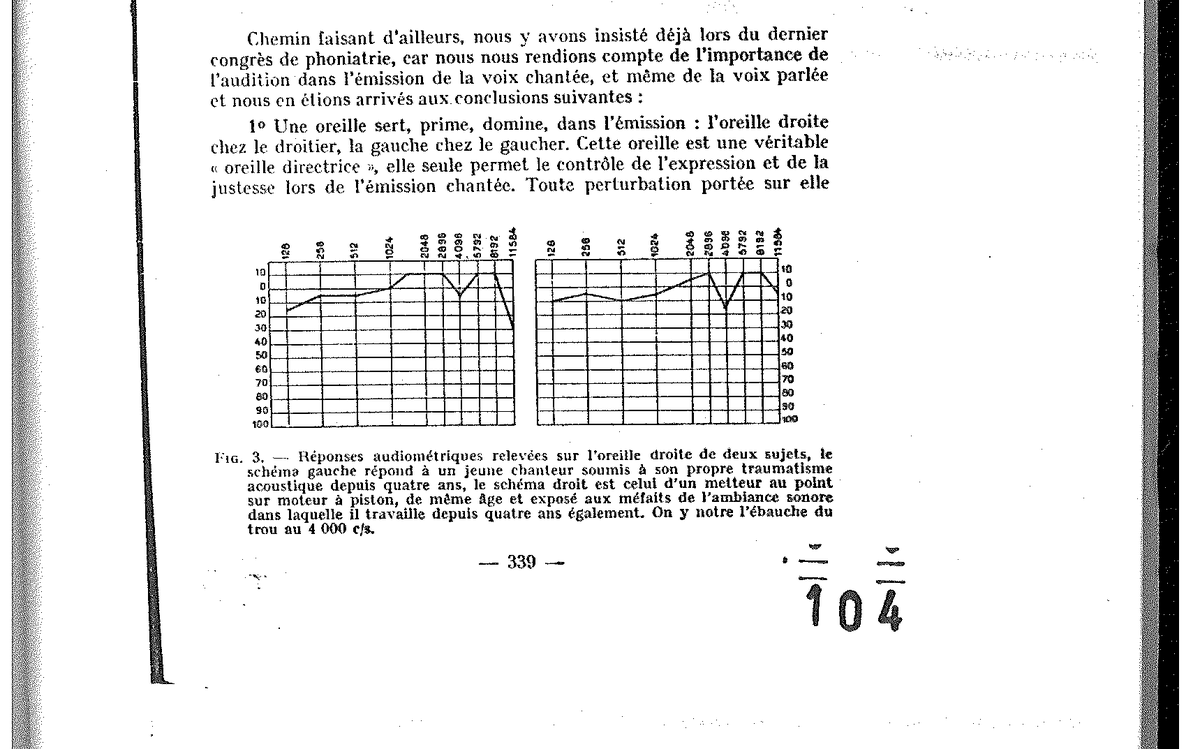
Fig. 3 — Audiometric responses taken on the right ear of two subjects — left diagram: young singer for 4 years (self-trauma), right diagram: tuner of piston engines (4 years in sonic environment). Sketch of the dip at 4,000 c/s.
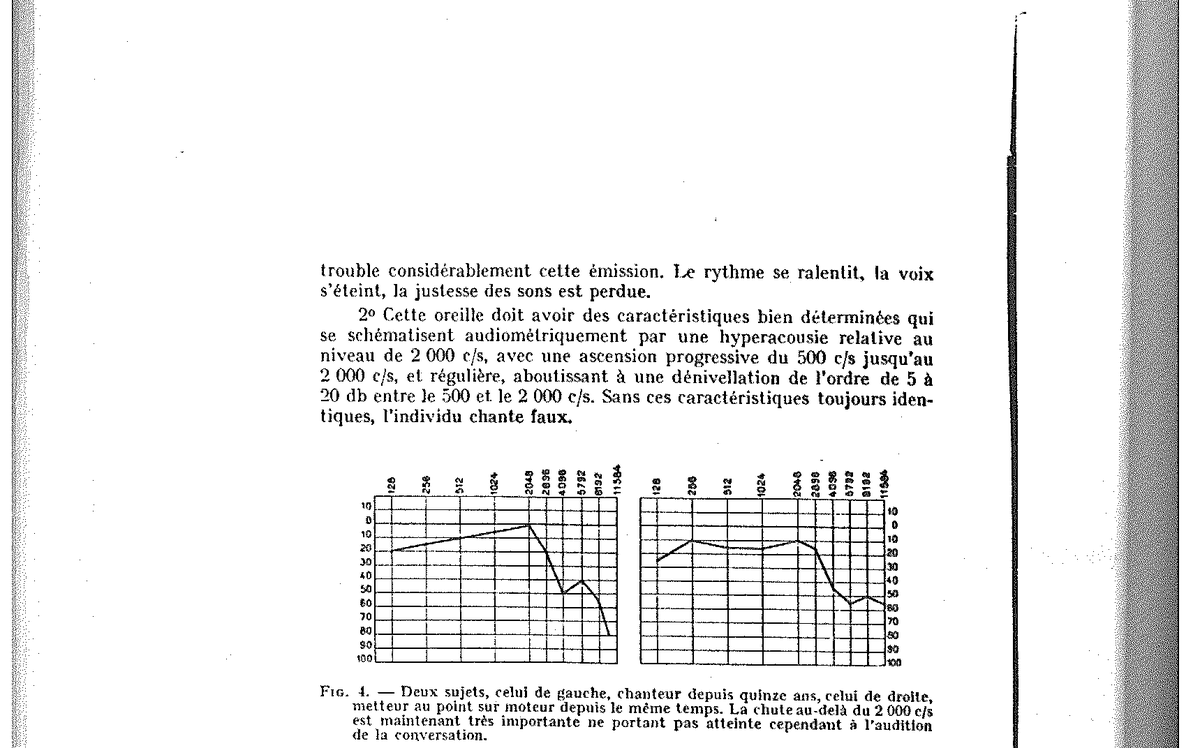
Fig. 4 — Two subjects: on the left, singer for 15 years; on the right, engine tuner for the same time. The fall beyond 2,000 c/s is very pronounced.
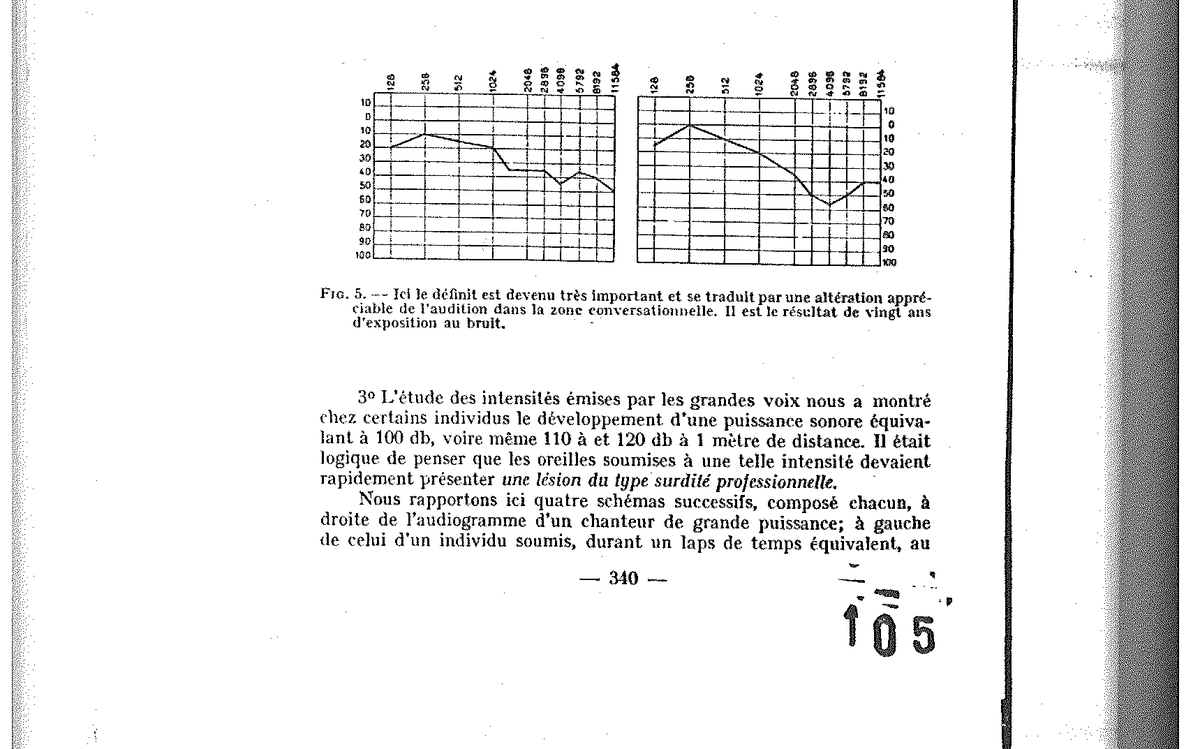
Fig. 5 — The deficit has become significant: appreciable alteration of hearing in the conversational zone, result of 20 years of exposure to noise.
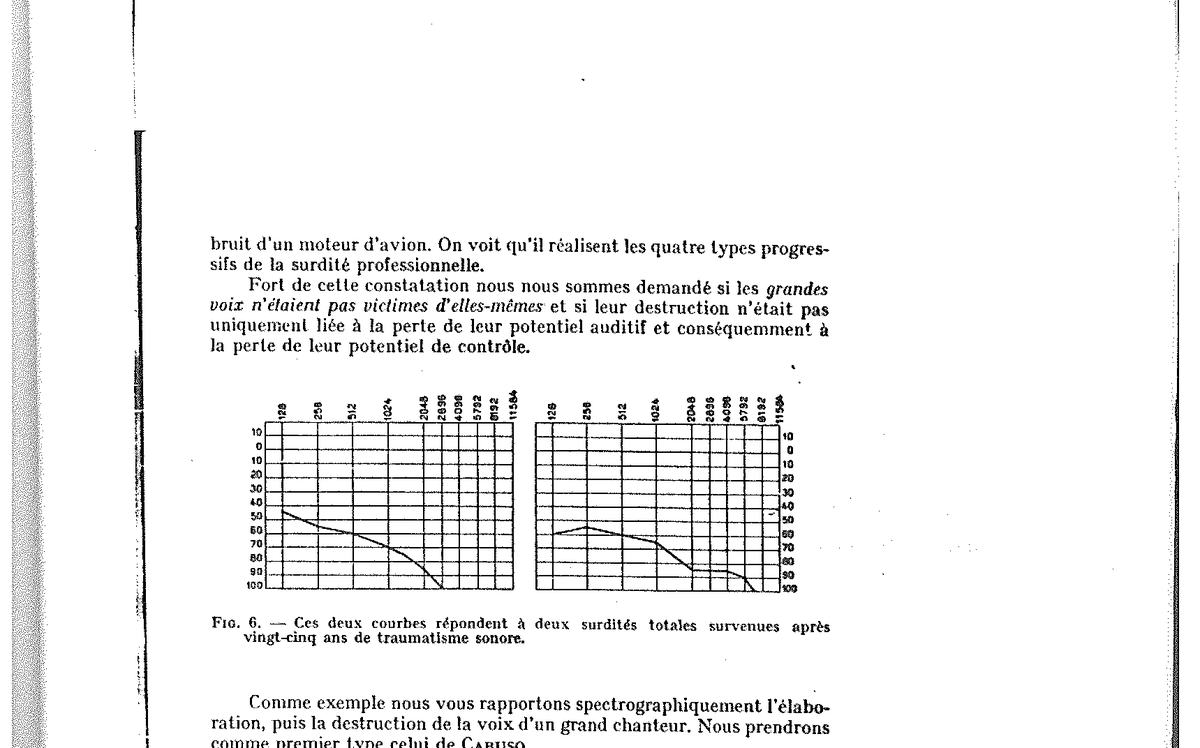
Fig. 6 — Two curves corresponding to two total deafnesses occurring after 25 years of sonic trauma.
VI. — Spectrography of Caruso’s voice (1901 - end of career)
To give these observations their full bearing, we have submitted to spectrographic analysis the whole of the recordings of Enrico Caruso preserved on cylinder and then on disc, from his first attempts of 1901 to the sessions preceding his death. This series, unique, allows a true spectral autopsy of the great voice.
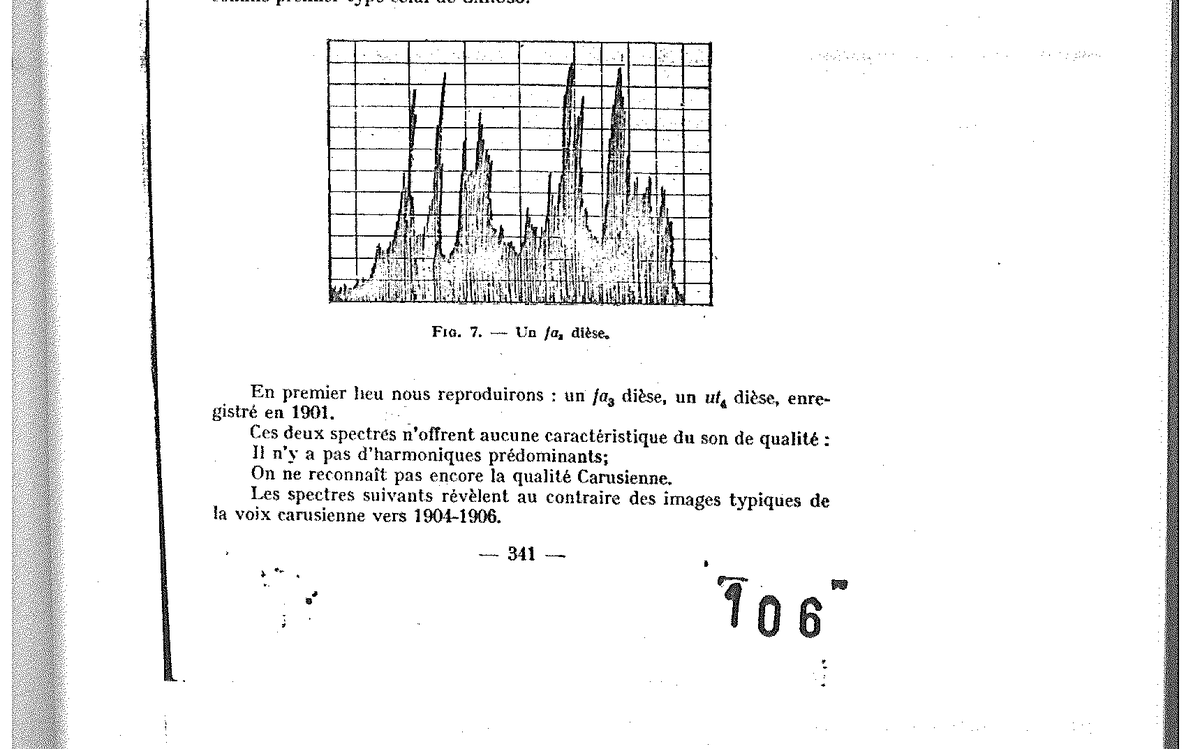
Fig. 7 — An F♯₃ — spectrogram.
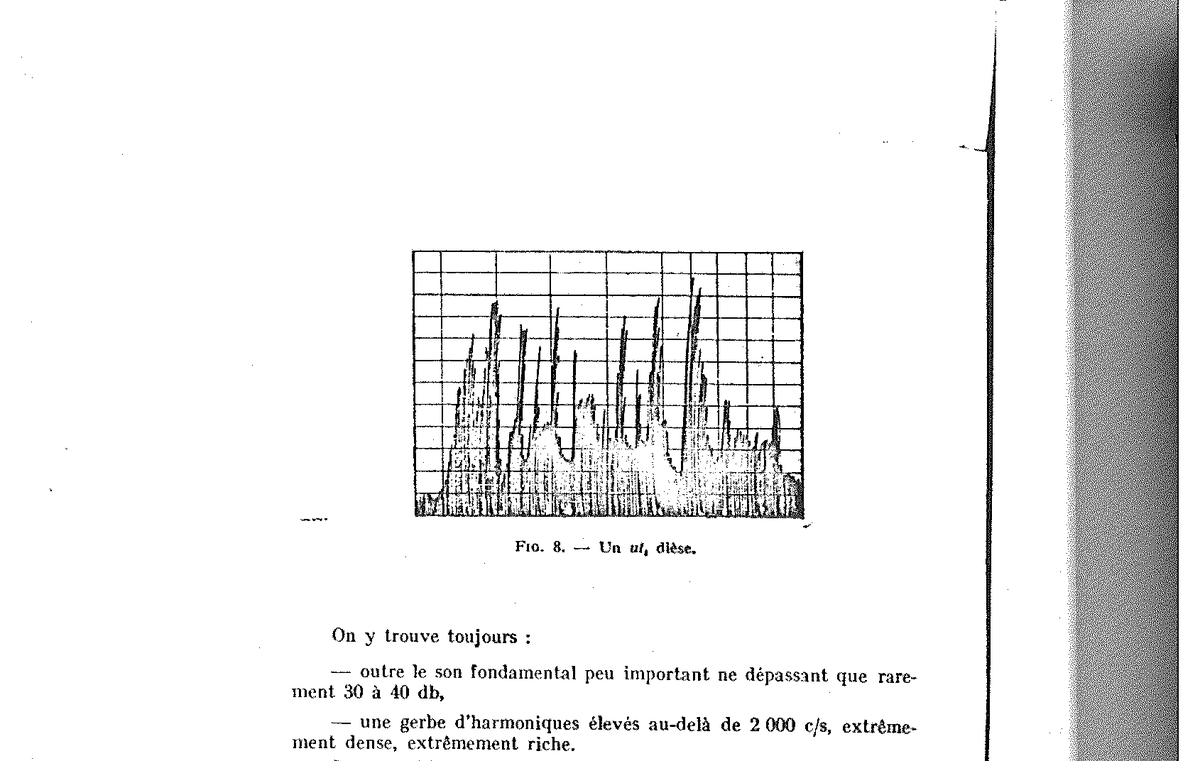
Fig. 8 — A C♯₄ — spectrogram.
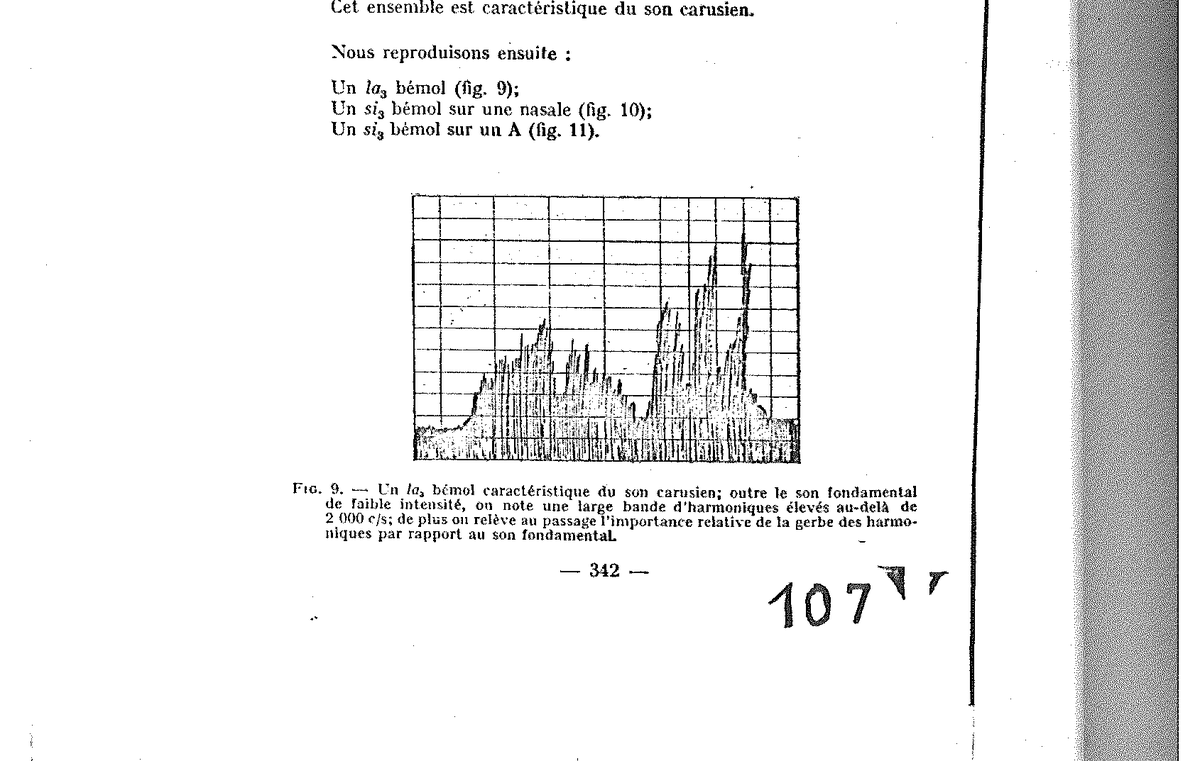
Fig. 9 — An A♭₃ characteristic of the Carusian sound: fundamental of weak intensity, broad band of high harmonics beyond 2,000 c/s, predominance of harmonics over the fundamental.
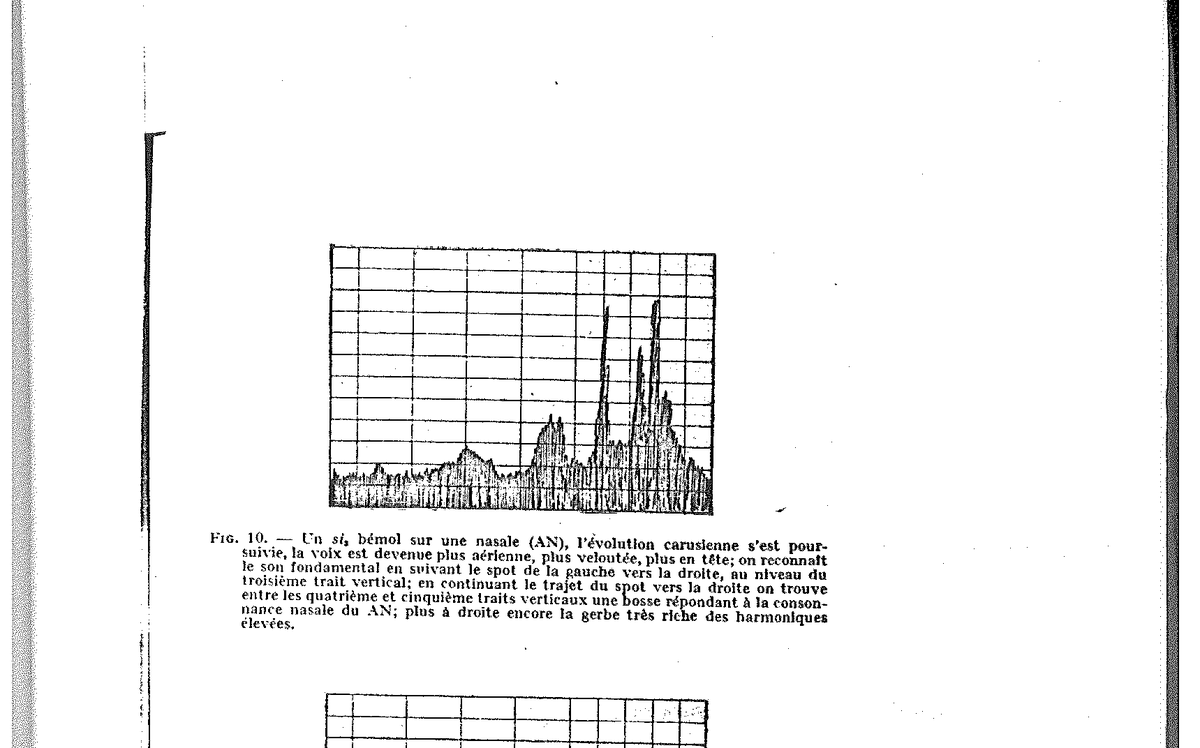
Fig. 10 — A B♭₃ on a nasal (AN) — the Carusian evolution has continued: a more aerial, more velvety, more head-resonant voice.
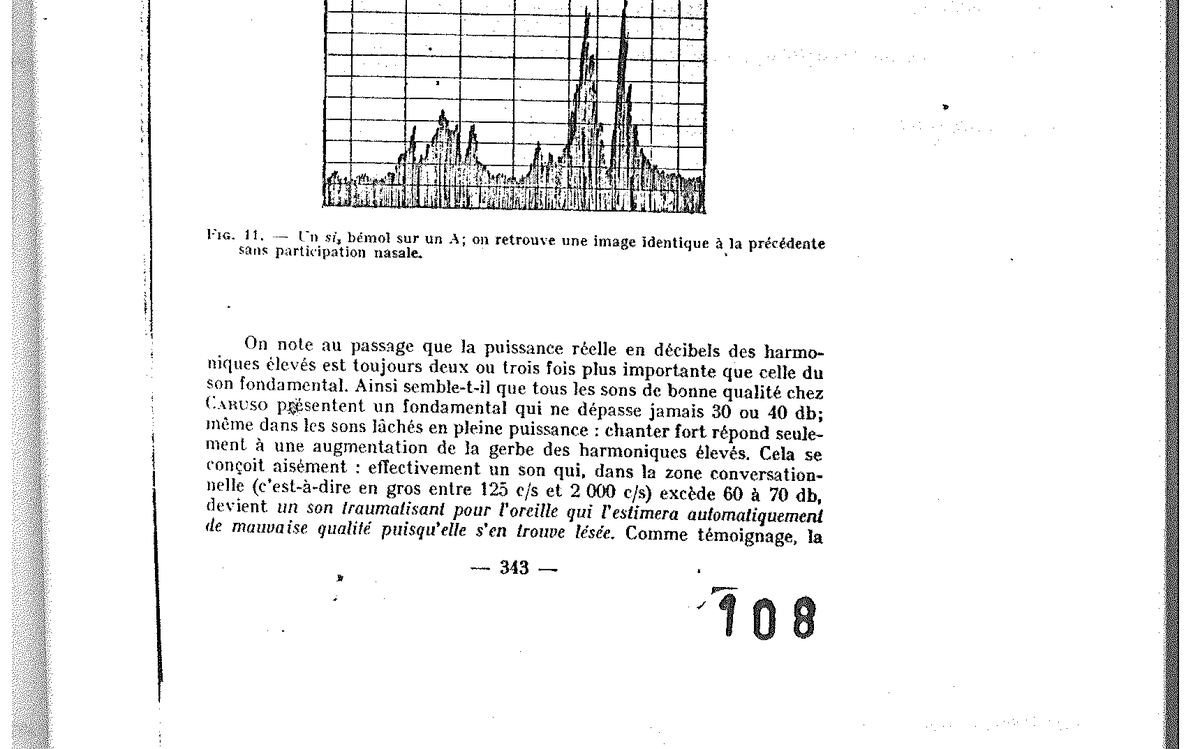
Fig. 11 — A B♭₃ on an A — image identical to the preceding one without nasal participation.
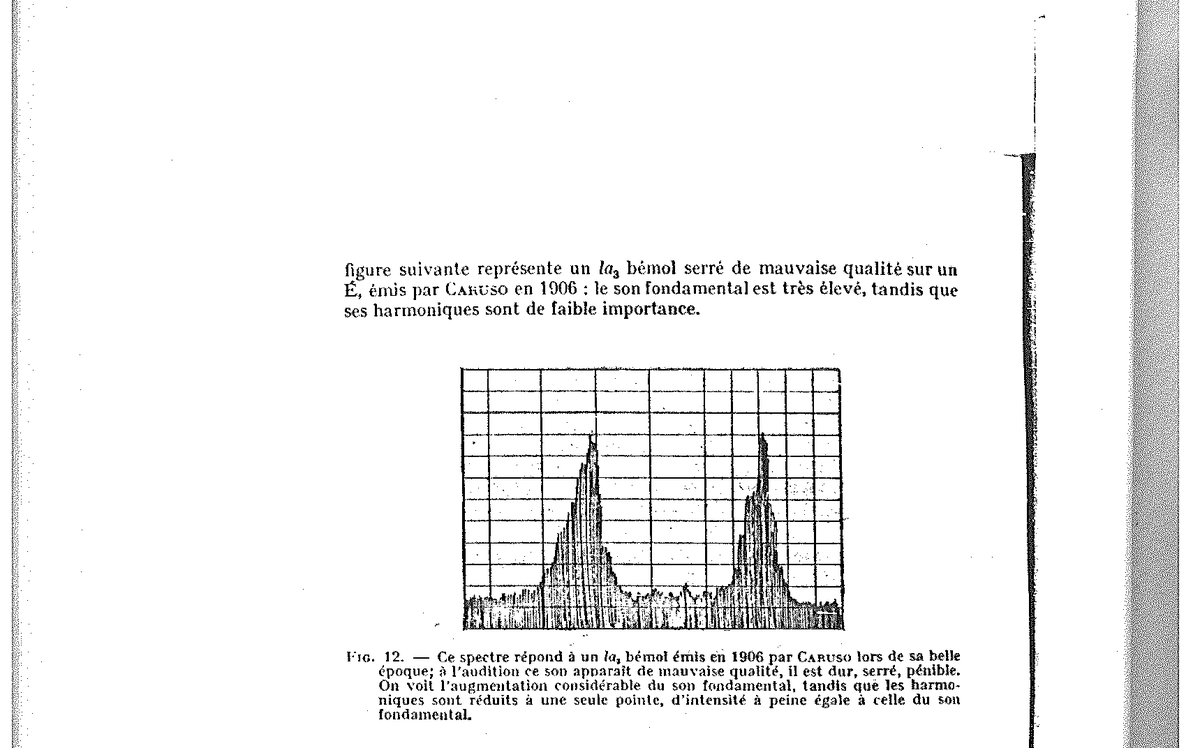
Fig. 12 — An A♭₃ emitted by Caruso in 1906 (golden age): considerable increase of the fundamental, reduced harmonics.
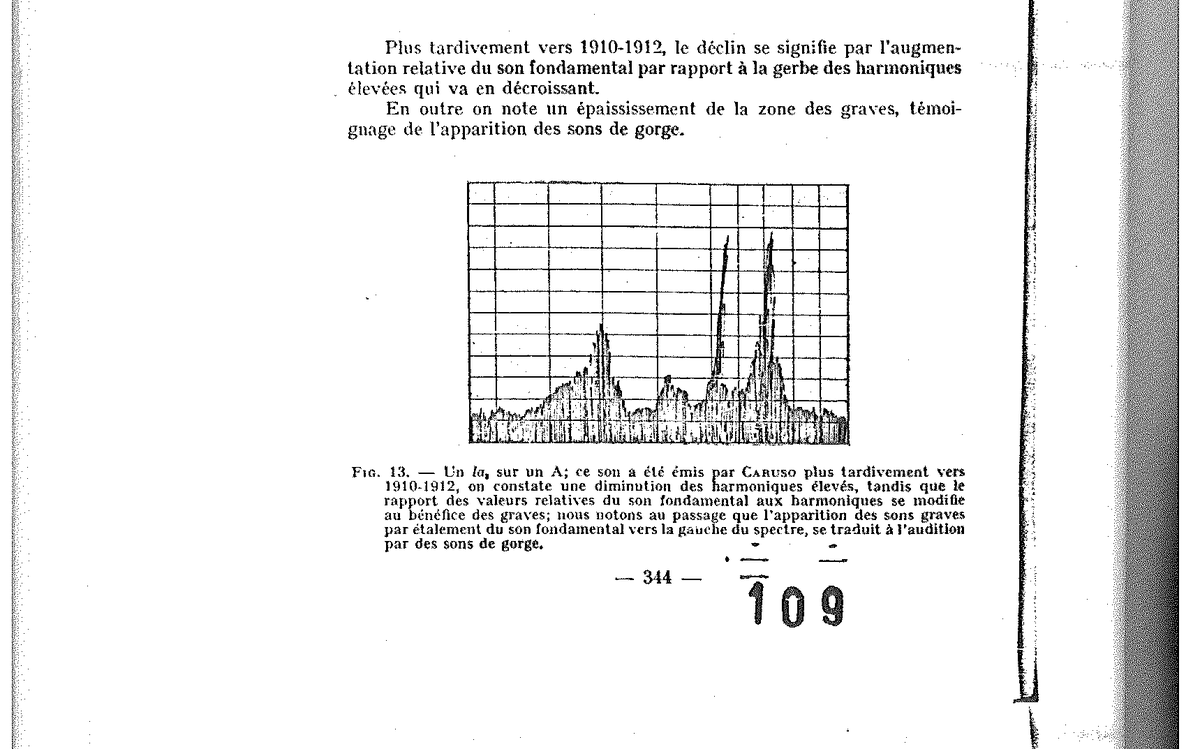
Fig. 13 — An A₃ on an A — Caruso later around 1910-1912: diminution of high harmonics, low sounds appearing through the spreading of the fundamental.
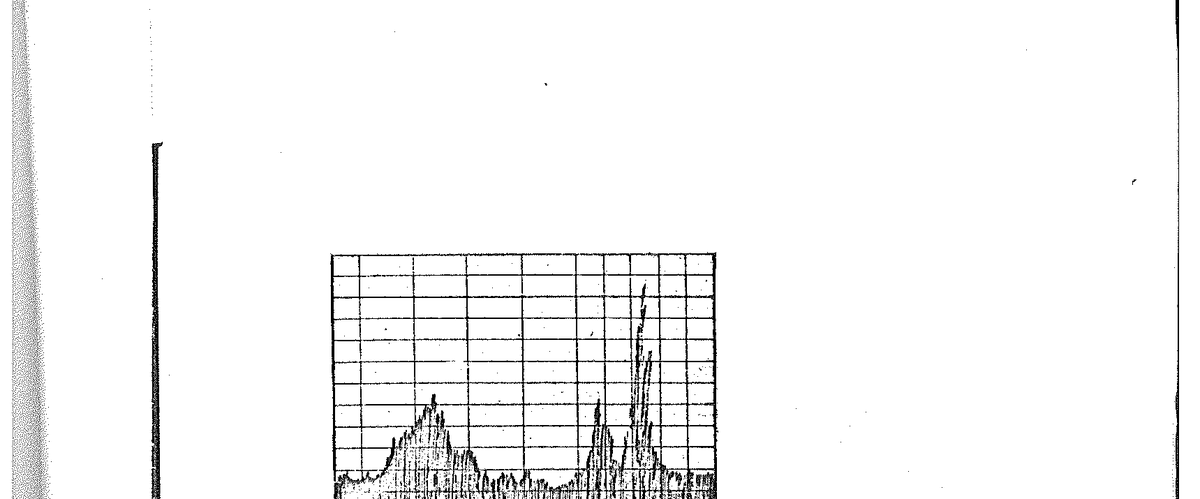
Fig. 14 — Still more typical, this A₃ on I: the high sheaf thins, throat sonorities grow.
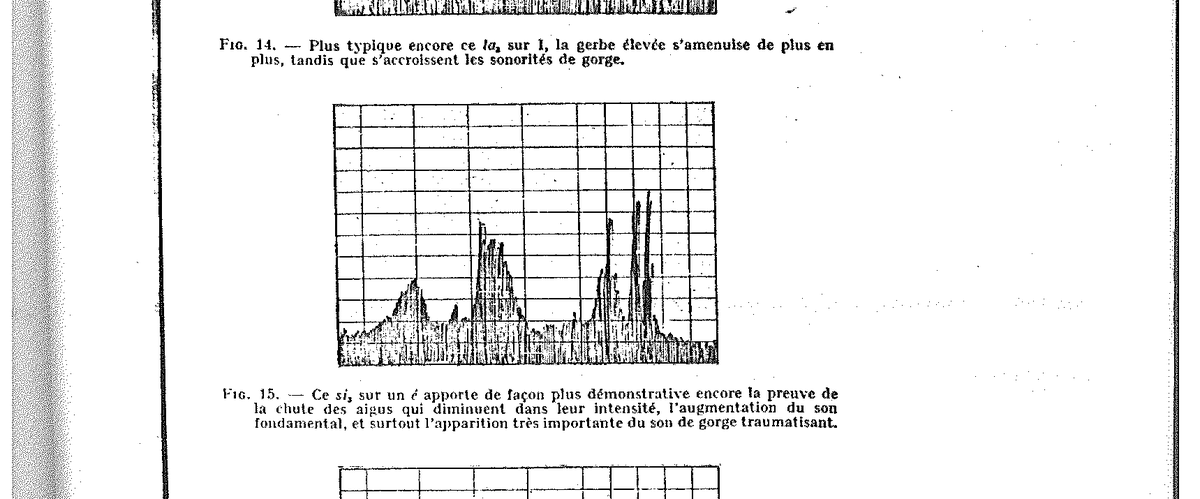
Fig. 15 — This B₃ on É brings the most conclusive proof of the fall of the highs, the increase of the fundamental, and the very pronounced appearance of the traumatising throat sound.
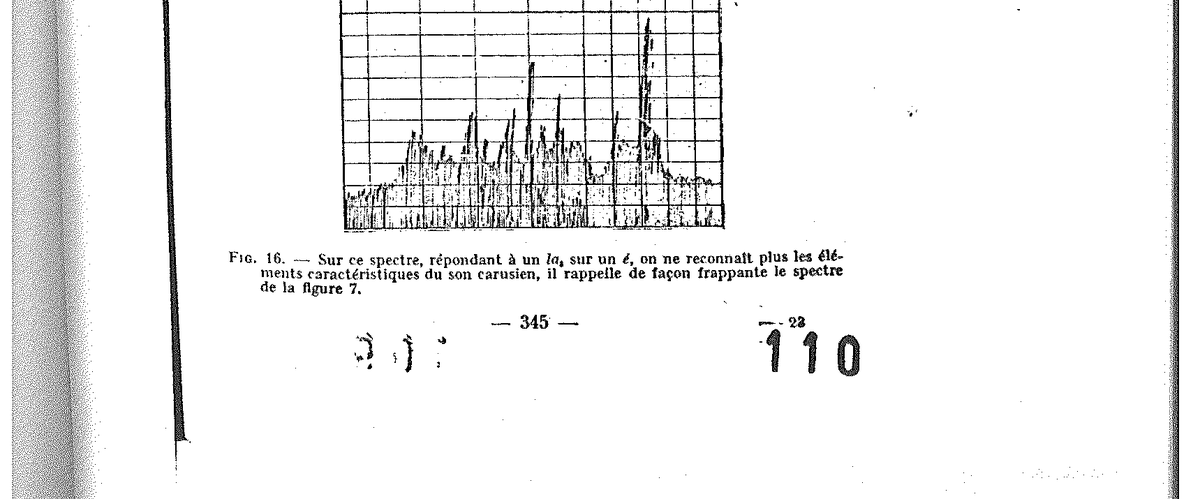
Fig. 16 — In this spectrum, corresponding to an A₃ on É, one no longer recognises the elements characteristic of the Carusian sound — it strikingly recalls the spectrum of figure 7.
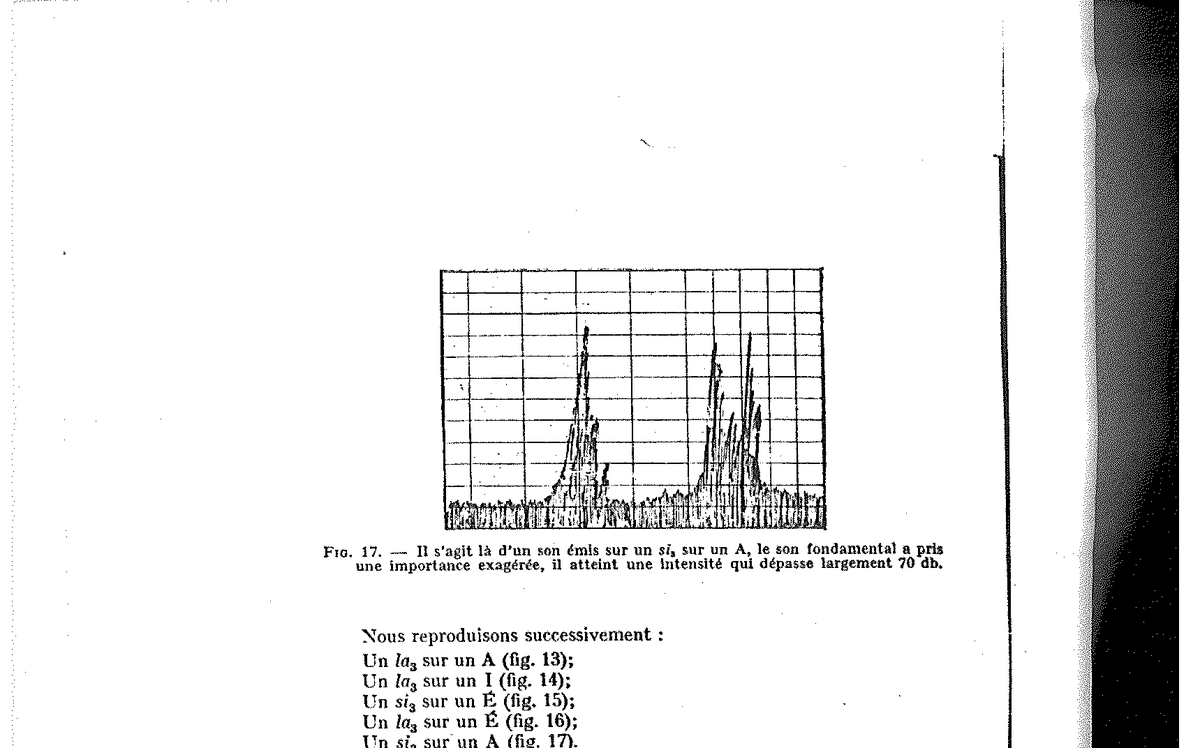
Fig. 17 — A sound emitted on a B₃ on an A: the fundamental has assumed an exaggerated importance, reaching an intensity largely exceeding 70 dB.
The lesson of this series is final: the deterioration of hearing entails a deterioration of the vocal spectrum, which is manifested by three signs — the fundamental swells, the high harmonics fade, nasal participation and throat sounds invade the emission.
VII. — Second example: a contemporary singer
To verify that what struck Caruso is not the privilege of an exceptional voice, we followed over several years a contemporary singer of international career, whose spectrographic evolution faithfully reproduces the scenario described above.
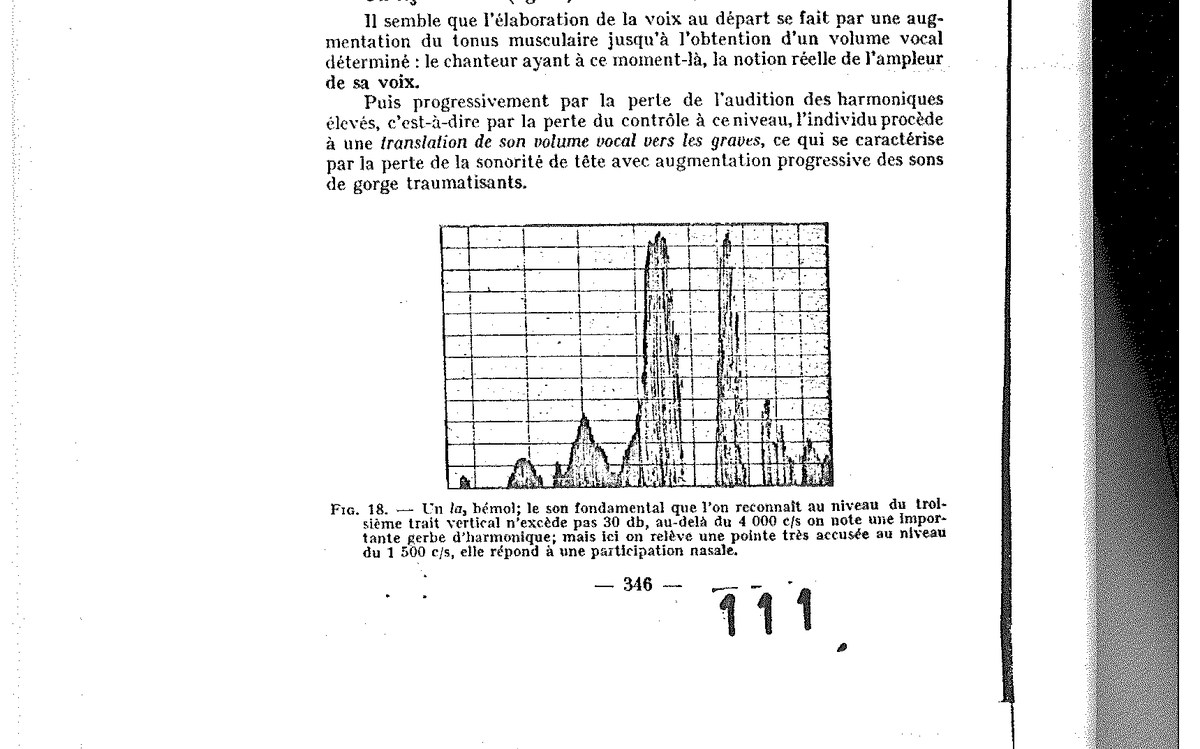
Fig. 18 — An A♭₃ (contemporary singer, start of career): fundamental not exceeding 30 dB, significant sheaf of harmonics beyond 4,000 c/s, peak at 1,500 c/s = nasal participation.
Fig. 19 — An F₃ on an A: same characteristics — slight fundamental, heavy participation of nasal resonances.
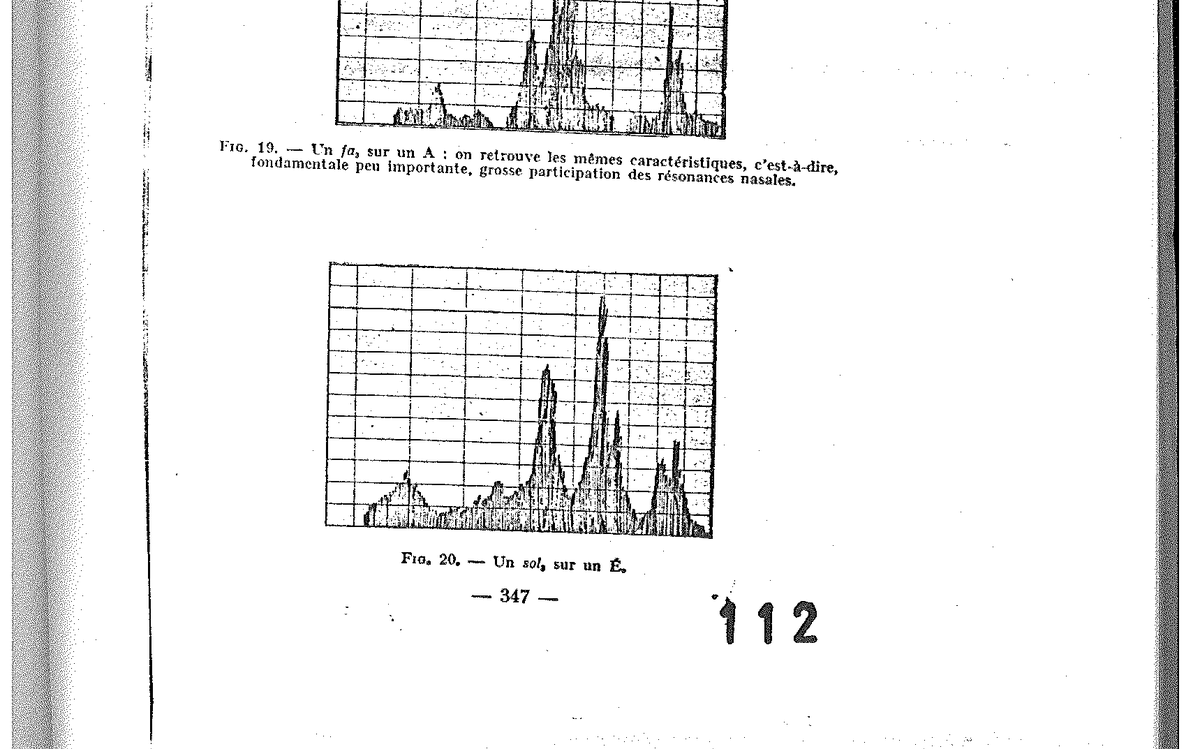
Fig. 20 — A G₃ on an É.
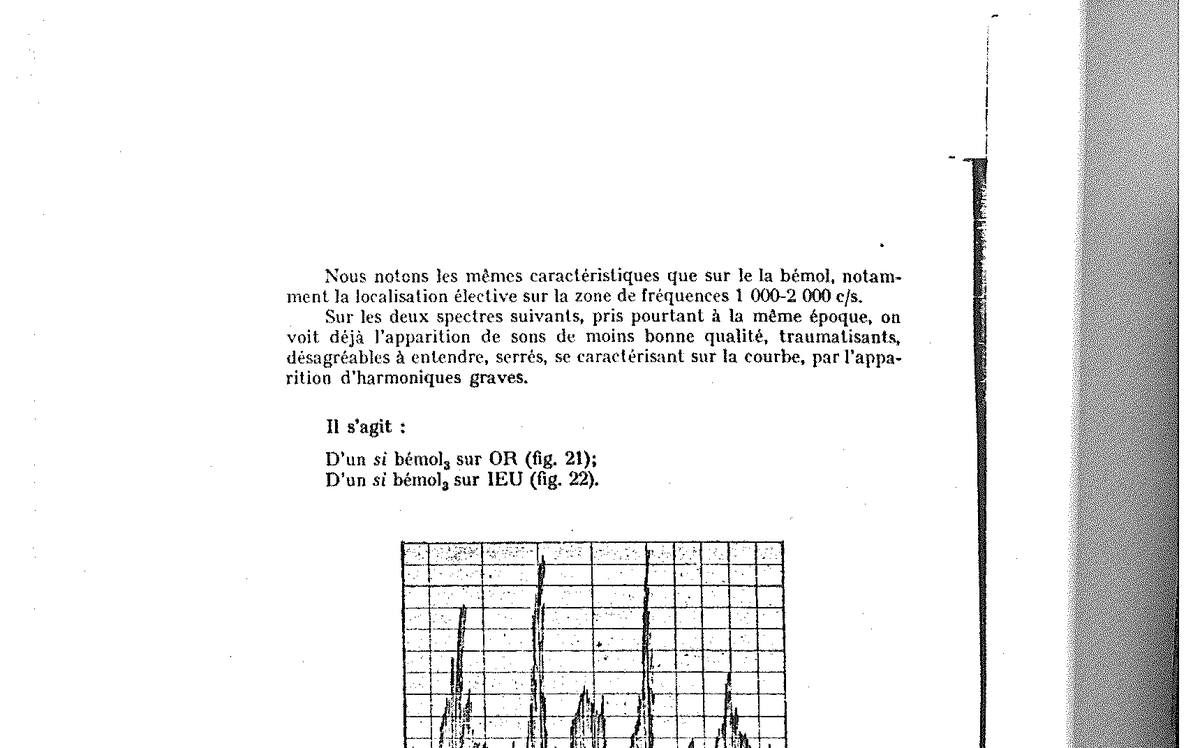
Fig. 21 — B♭₃ on an OR (golden age of this singer): tight, forced sound; peak at 300 c/s (throat support), then fundamental too intense relative to its associated high harmonic.
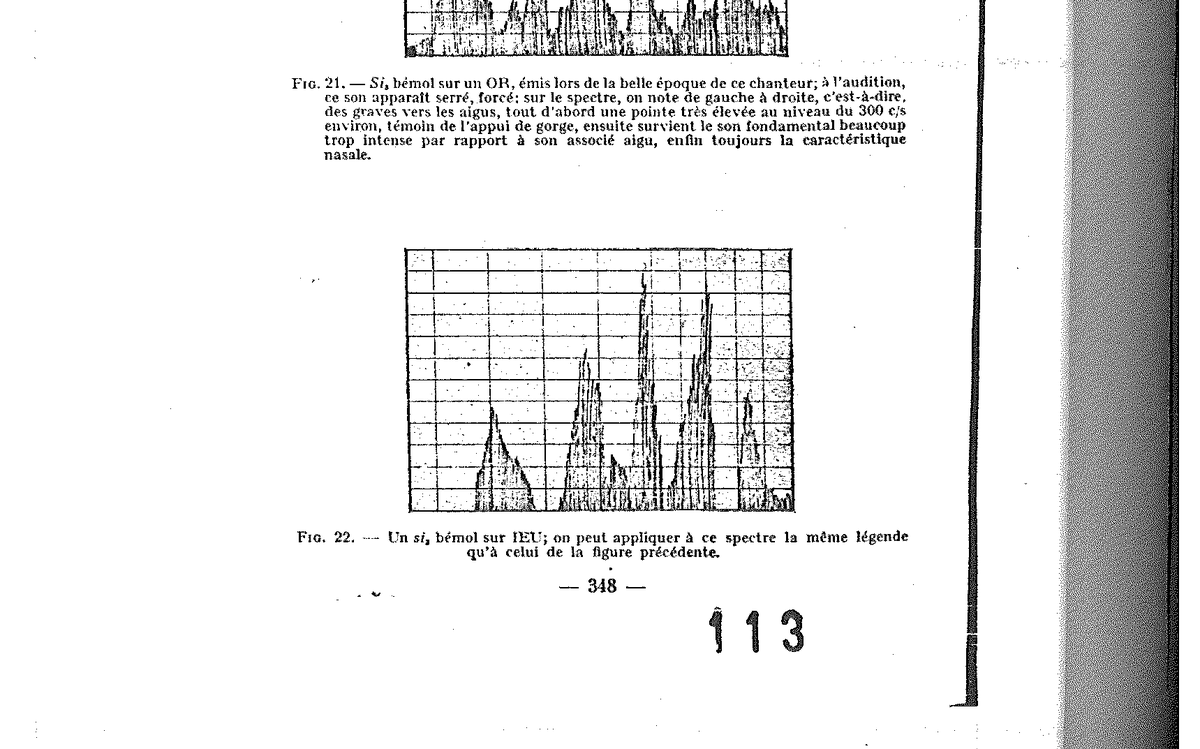
Fig. 22 — A B♭₃ on IEU — same caption as the previous figure.
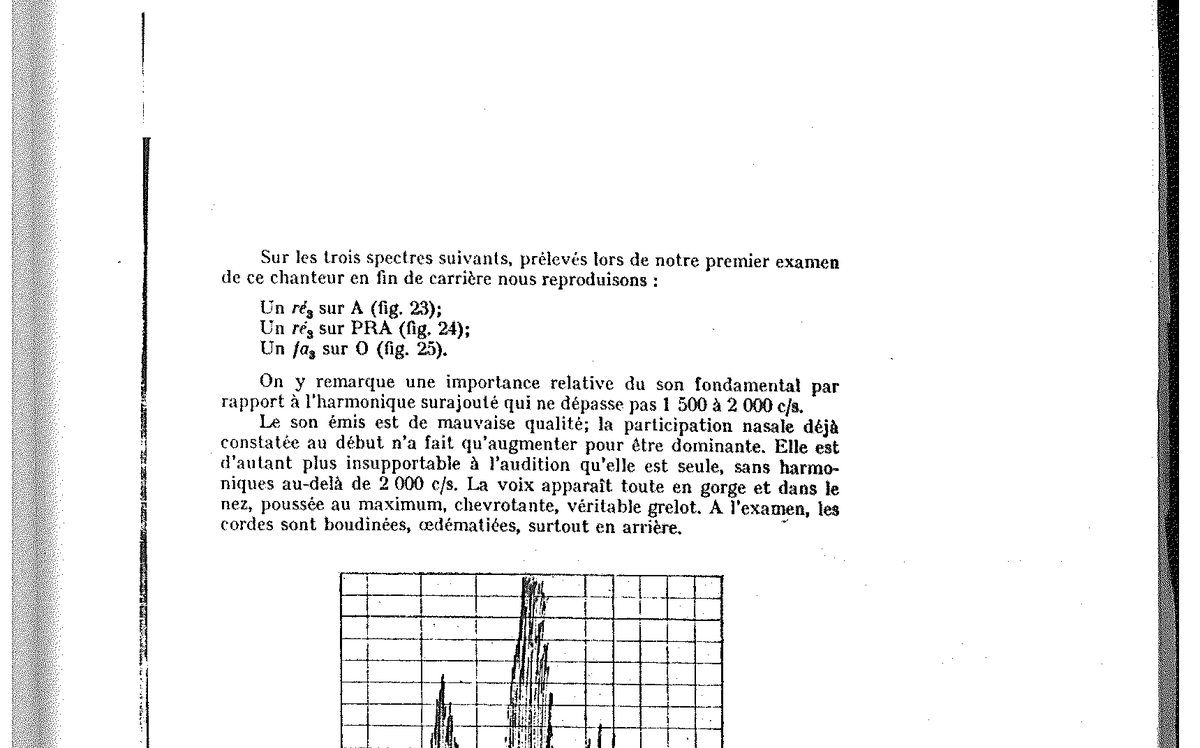
Fig. 23 — A D₃ on an A emitted by this singer at the end of his career: increase of the fundamental, predominant nasal participation, no harmonics whatsoever beyond 2,000 c/s.
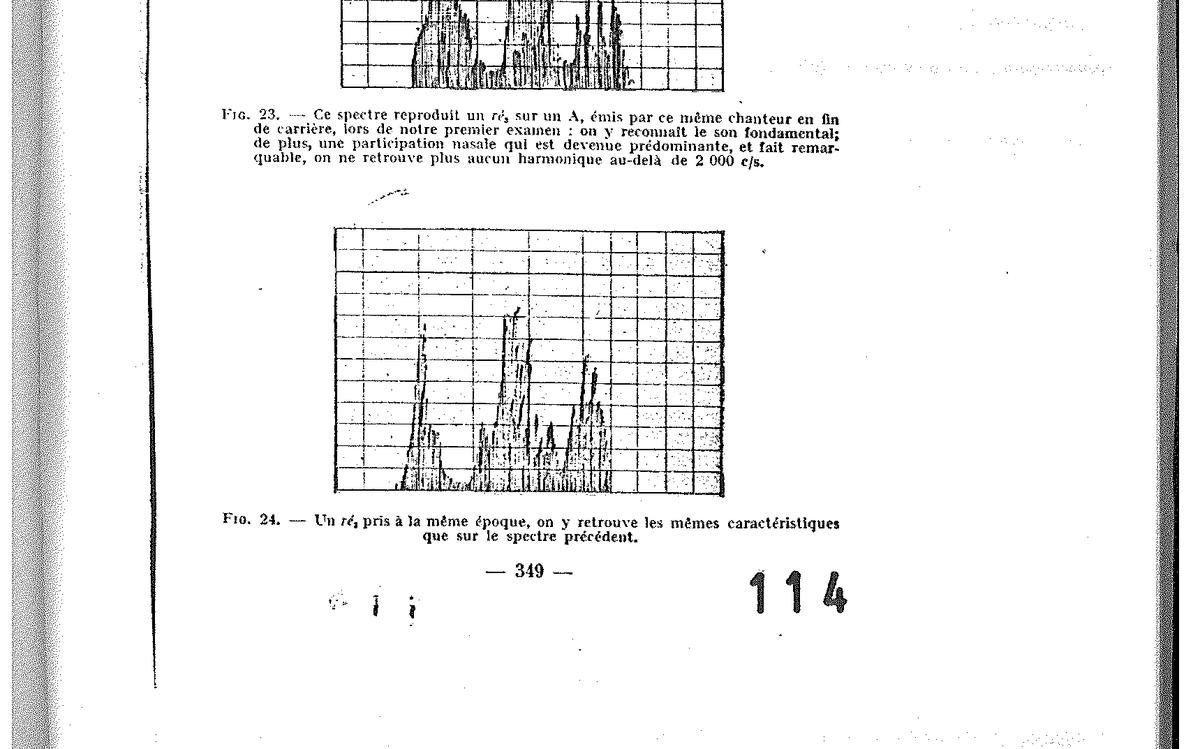
Fig. 24 — A D₃ taken at the same period — same characteristics as the previous spectrum.
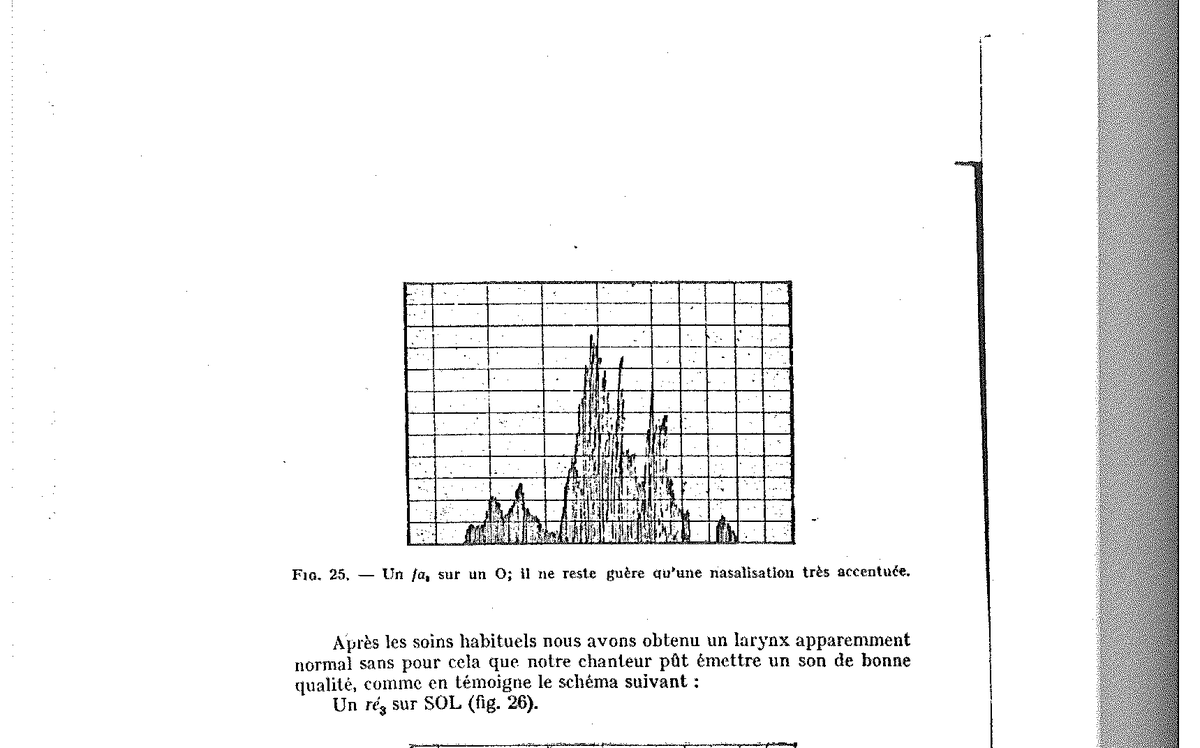
Fig. 25 — An F₃ on an O: hardly anything remains but a very pronounced nasalisation.
VIII. — Therapeutic restoration
The therapeutic application of our method then consists in restoring the audiogram — by medical care (placental extract, vitamin C, high-dose vitamin B), then by experimental re-education of the ear by means of filters — in order to see the vocal spectrum return spontaneously to its earlier configuration.
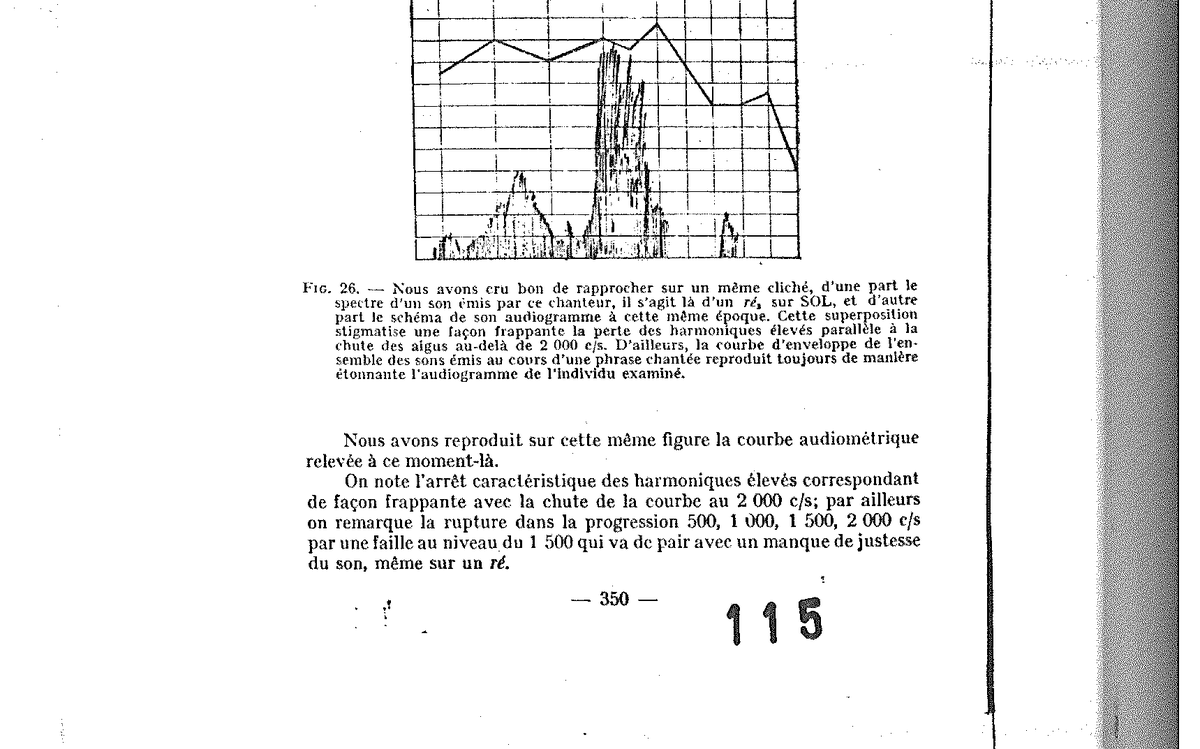
Fig. 26 — A D₃ on SOL with the spectrum of the emitted sound and the singer’s audiogram superposed — the loss of harmonics beyond 2,000 c/s is parallel to the fall of the curve.
We have applied ourselves to reproducing in this singer an audition identical to that given by the envelope curve of the earlier spectra and, in addition to the care made up of placental extract, vitamin C and high-dose vitamin B, we have re-educated his ear by considering, as we have seen above, that the destruction of the voice occurred at a given moment with the appearance of low sounds, the only zone of audition still controlled. We wondered whether, by suppressing these traumatising harmonics through a system of filters during the monitoring of the sung voice, we might not obtain an inverse translation of the whole vocal volume, towards the high frequencies: this is what experience confirmed for us.
The result is immediate; from the outset the individual sings without pushing, the accuracy of his sound reappears at the same time as the quality of former times is recovered.
Fig. 27 — Spectrum gathered immediately upon the experimental modification of the subject’s ear: fundamental of good quality, slight nasal participation, arrow of harmonics towards 3,000 c/s.
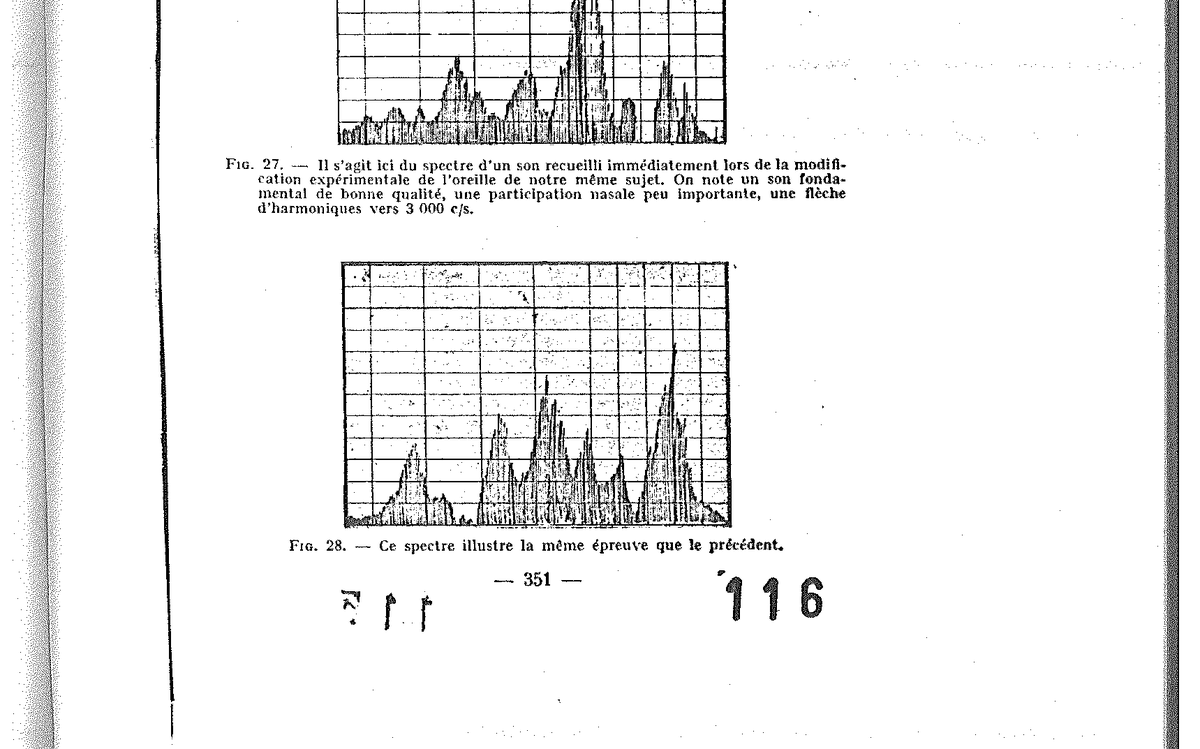
Fig. 28 — Spectrum illustrating the same trial as the preceding one.
IX. — The re-education apparatus
The re-education is performed simply as we have presented it in the practical works, thanks to our apparatus whose diagram we reproduce below.
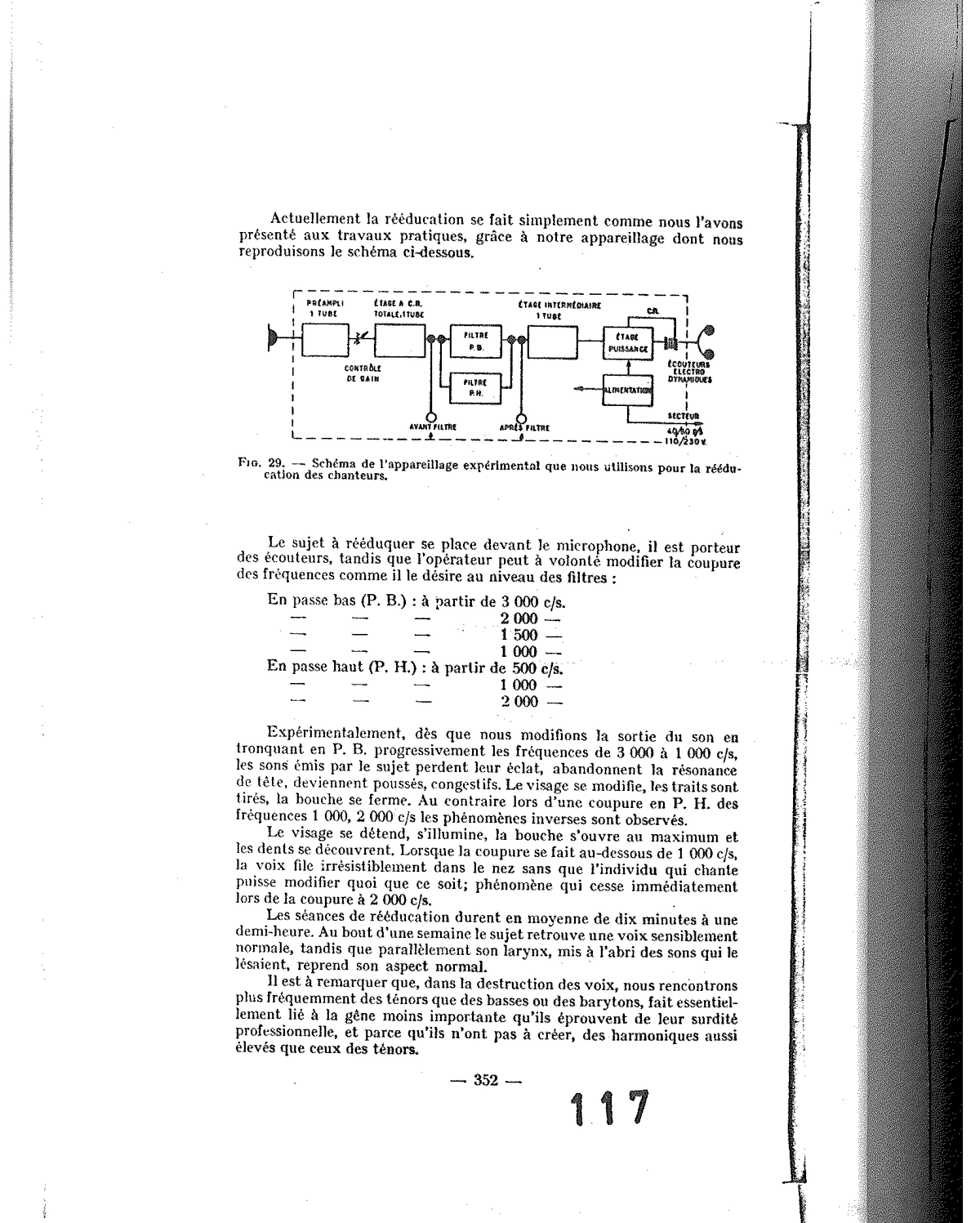
Fig. 29 — Diagram of the experimental apparatus used for the re-education of singers: pre-amplifier, C.R. stage, intermediate stage with P.B. and P.H. filters, power stage, electrodynamic earphones (mains 110/230 V).
The subject to be re-educated stands before the microphone and wears the earphones, while the operator can at will modify the cut-off of the frequencies:
-
In low-pass (P.B.): from 3,000 c/s, 2,000, 1,500 and 1,000 c/s.
-
In high-pass (P.H.): from 500, 1,000 and 2,000 c/s.
Experimentally, as soon as we modify the output of the sound by progressively truncating in P.B. the frequencies from 3,000 to 1,000 c/s, the sounds emitted by the subject lose their brilliance, become head resonance, become pushed, congested. The face changes, the features are drawn, the mouth closes. By contrast, with a cut-off in P.H. of frequencies 1,000 and 2,000 c/s, the inverse phenomena are observed. The voice loosens, lightens, the mouth opens to the maximum and the features uncover. When the cut-off is made above 2,000 c/s, the voice loses its life in the nose and the singing individual cannot modify anything at all; a phenomenon which ceases immediately upon a cut-off at 2,000 c/s.
The re-education sessions last on average ten minutes to half an hour. After a week of treatments at the rate of ten sessions a day, we see the subject recover a substantially normal voice, while in parallel his larynx, sheltered from the sounds that were lesioning it, resumes its normal aspect.
It should be noted that, in the destruction of voices, we more frequently encounter tenors than basses or baritones. This is essentially linked to the more significant inconvenience they experience from their occupational deafness, and because they do not have to create, in their need to rise, harmonics as elevated as those of tenors.
X. — Conclusion
Finally to conclude, let us note that this research is not devoid of all distraction. We were able to have you hear a black singer at the practical demonstrations — a perfect pianist, a good composer, who came to consult us to learn his vocal possibilities. He presented at examination a normal larynx, a normal rhino-pharynx, an audiogram very atypical for a singer. According to our conception, it was impossible for him to sing in tune. We first asked him to perform a “negro spiritual”: he already displayed many difficulties in the accurate expression of his voice. We then asked him for a European air, and it was frankly impossible, at least until halfway through the piece performed, to recognise the melody our artist had chosen.
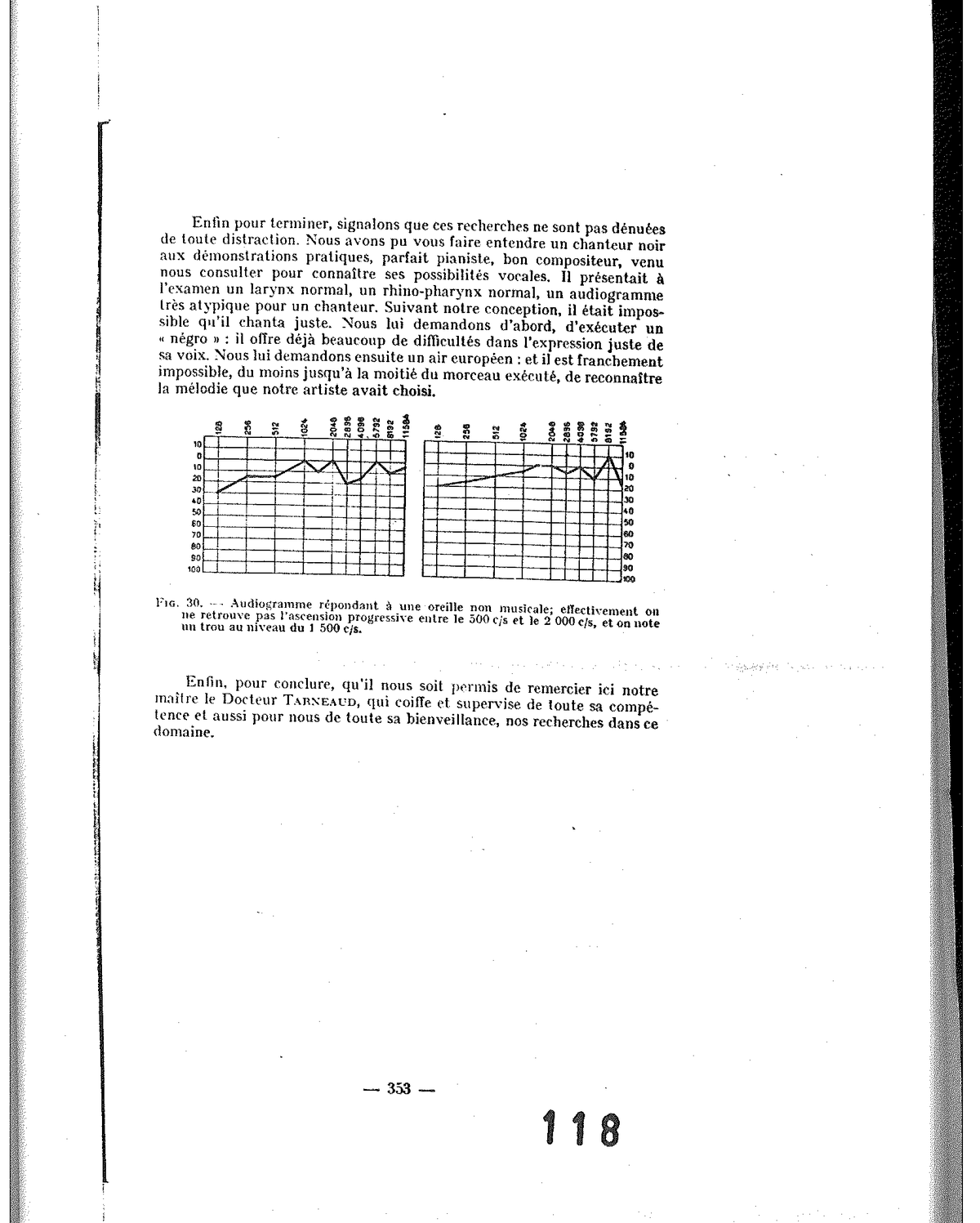
Fig. 30 — Audiogram corresponding to a non-musical ear: no progressive ascent between 500 and 2,000 c/s; dip at 1,500 c/s.
Finally, by way of conclusion, may it be permitted to us to thank here our master, Doctor Tarneaud, who oversees and supervises with all his competence — and also for us with all his benevolence — our research in this field.
Source: Tomatis A., “La correction de la voix chantée”, offprint, pp. 335-353 (nineteen pages, thirty figures). Work conducted at the Research Laboratory of the S.F.E.C.M.A.S. (Société Française d’Étude et de Construction de Matériel Aéronautique Spécial, Arsenal de l’Aéronautique). Digitised document from Alfred Tomatis’s personal archives.